Fifty consecutive parturientes from June 2014 to May 2017 were retrospectively selected.
Inclusion criteria were: placenta previa and/or ultrasound suspect of PAS, availability of MR imaging and surgery outcome/pathology.
Among the fifty potentially eligible patients,
12 were excluded because of parturients moved to other institutions before the delivery (n=9),
emergency delivery before MR exam (n=1),
vaginal delivery (n=1),
absence of placenta previa on MRI (n=1).
Finally,
a total of 38 patients (median age of 36 years; range 21-44) were included (Fig.1).

Fig. 1: Figure 1. Flowchart of the study population.
All the MR exams were performed within a week from the US examination on a 1.5T scanner.
MR protocol comprised T2w images (including high resolution sequences) in sagittal,
coronal and axial orientations by using a fast spin-echo sequence; T1-thrive were obtained in axial plane.
Thirty-eight placental MRI exams were reviewed by two radiologists in consensus,
assessing the following features (Fig.2): the presence of intraplacental T2 dark bands (Fig.2a),
myometrial thinning (Fig.2b),
intraplacental abnormal vascularization (Fig.2c),
uterine bulging (Fig.2d),
heterogeneous intraplacental sign (Fig.2e),
placental protrusion sign (Fig.2f),
placental recess (Fig.2g),
percretism sign (Fig.2h).
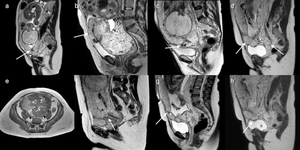
Fig. 2: Figure 2. Sagittal T2-weighted (a-d, f-h) and axial T1-weighted (e) images showing MRI criteria. a Intraplacental dark band (white arrow) with the major diameter longest than 2 cm. b Myometrial thinning (white arrow): focal defect of the hypointense uteroplacental interface with myometrial thinning or indistinctness of myometrial delineation. c Intraplacental abnormal vascularity: enlarged and tortuous vessels (white arrow) with a diameter > 6 mm. d Uterine bulging (white arrows): loss of normal “pear shape” of the uterus, with the wider appearance of the body than the caudal segments. e Heterogeneous intraplacental sign: heterogeneous intensity within the placenta due to hemorrhage or vascular lacunae (white asterisks). f Placental protrusion sign: the placenta extends and projects (white arrow) into the internal uterine os. g Placental recess: the contraction of the flow placental (white arrow) surface accompanying a dark band (white asterisk). h Percretism signs: direct invasion (white arrow) of bladder (B).
The presence of each MR sign was qualitatively assessed according 5-points scale: 1=absent,
2=probably absent,
3= indeterminate,
4=probably present,
5=certainly present.
In case of disagreement between the two readers,
a third radiologist decided the final score.
Both “pathology reports” and “clinical intrapartum findings” were used as standard of reference to confirm the presence of invasive placenta.
A multidisciplanary team consensus based on clinically records established the clinical outcome.
In detail,
a poor outcome group was defined as parturient with massive intrapartum/peripartum bleeding (>1000ml) and/or emergency hysterectomy.
The good outcome group was defined as parturient with minor intrapartum/peripartum hemorrhage (≤1000ml) and preserved uterus.
The frequency distribution of qualitative MRI features regarding presence/absence and poor/good clinical outcome was calculated by using Fisher exact test.
The diagnostic power of each MR feature was calculated by receiver operating characteristic (ROC) curve analysis.
All the MR features were included in a stepwise discriminant function analysis.
This analysis was conducted to determine whether a set of variables is effective in predictive category membership.
Coefficients were also determined indicating the unique contribution of each variable to predictive function.
Finally,
a ROC curve analysis of predictive function (both for invasive placenta and for clinical outcome) was used to determine a cutoff with relative sensitivity and specificity.


 and axial T1-weighted (e) images showing MRI criteria. a Intraplacental dark band (white arrow) with the major diameter longest than 2 cm. b Myometrial thinning (white arrow): focal defect of the hypointense uteroplacental interface with myometrial thinning or indistinctness of myometrial delineation. c Intraplacental abnormal vascularity: enlarged and tortuous vessels (white arrow) with a diameter > 6 mm. d Uterine bulging (white arrows): loss of normal “pear shape” of the uterus, with the wider appearance of the body than the caudal segments. e Heterogeneous intraplacental sign: heterogeneous intensity within the placenta due to hemorrhage or vascular lacunae (white asterisks). f Placental protrusion sign: the placenta extends and projects (white arrow) into the internal uterine os. g Placental recess: the contraction of the flow placental (white arrow) surface accompanying a dark band (white asterisk). h Percretism signs: direct invasion (white arrow) of bladder (B).")