Ferumoxytol as a dual contrast agent
- Ferumoxytol is the injectable solution of ultrasmall super-paramagnetic iron oxide (USPIO) nanoparticle ferumoxide,
used for the treatment of iron deficiency anemia in patients with chronic renal insufficiency.
- Ferumoxytol functions as a dual relaxation MR contrast agent providing high signal intensity (SI) with short echo times (TE),
and lower signal with longer TE due to its high R2* relaxivity on T1 weighted images.
- With the intravascular blood pool signal suppressed,
intralymphatic gadolinium can easily be distinguished since venous contamination with gadolinium would also be suppressed by the presence of intravascular ferumoxytol.
--------------------------------------------------------------------------------------------------------
MR venogram: short TE (<5msec @3T) = high SI of ferumoxytol/blood
MR lymphangiogram: long TE (>5msec @3T) = low SI of ferumoxytol/blood
→ blood pool is selectively eliminated ("turned off")
→ intralymphatic gadolinium stands out ("lymphatic map")
___________________________________________________________
Mechanism of blood pool suppression with ferumoxytol
At equilibrium blood concentration ferumoxytol markedly shortens T2* of the blood (achieving T2* of the blood pool of less than approximately 2.0 msec).
Various echo times are needed to determine the best individual ferumoxytol suppression on T1 gradient echo images.
USPIO Enhanced MR Lymphangiography - Contrast Administration
- Approximately 30 minutes prior to the interstitial gadolinium injection ferumoxytol at a dose of 5 mg iron per kilogram of body weight (diluted with normal saline to a total volume of 60 mL) is slowly administered intravenously at a rate of 0.1 mL/sec (over ≥15minutes).
Monitoring is mandatory during this time period.
- Selection of echo times on T1 weighted gradient echo imaging is crucial for the desired imaging effects (combined MRV/MRL versus MRL)
- The interstitial injection technique of gadolinium for ferumoxytol enhanced and conventional MRL technique is identical.
- The image acquisition protocol for USPIO enhanced MRL differs from the conventional MRL technique:
USPIO Enhanced MR Lymphangiography - Imaging Protocol
3D T2 FS and volumetric calculations remain the same as in the conventional MRL.
Key differences to conventional MRL (introduced by Maki et al.
2016) for:
- Low-resolution TE scout with 5 different TE pairs (3D-mDixon T1 GRE)
- Selection of the best TE pair to completely suppress ferumoxytol signal in blood vessels,
mostly between 4 and 8ms,
without causing suppression of gadolinium signal in lymphatics
- Dynamic multistation high-resolution 3D-mDixon T1 GRE (mostly in sagittal orientation) with above selected TE pair every 5–10 minutes for 50–70 minutes.
Imaging at 20min and 45-50-min depicts most lymphatic channels (Fig. 11)
- Final axial 3D-mDixon T1 GRE over the shoulder/axilla for upper and over the pelvis including the aortic bifurcation for lower extremities using a short TE pair (for combined MRV/MRL) and a longer TE pair (for MRL) to depict enhancing lymph nodes (Fig. 13).
Nodal enhancement would confirm an adequate delay of the last dynamic time point (for example 50min).
- Combined MRV/MRL: 3D GRE T1- weighted pulse sequences do not require intravenous administration of gadolinium as a contrast agent,
but take advantage of the relaxivity effects of ferumoxytol with short echo times.
The interstitially injected gadolinium within lymphatics is also visible but present next to arteries and veins,
similar to the effect of a separate intravascular gadolinium injection.

Fig. 11: Effect of long echo pairs on blood pool suppression on ferumoxytol enhanced mDixon T1 weighted gradient echo images after intradermal administration of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% into the interdigital web spaces (multistation MIPs reconstructed from high resolution sagittal source images):
A) MRV/MRL (short TE pair) shows veins besides areas of dermal backflow (arrowheads) as a sign of lymphatic obstruction. Dynamic MR lymphangiograms at four different time points (B-E) with increasing TE pairs demonstrate lymphatics more efficiently through signal suppression of blood pool with longer echo times. Note that short segments of signalintense slow or stagnating blood flow with poor admixture of ferumoxytol (curved arrows) could be successfully eliminated with a longer TE pair of 6.2/7.4ms and repeated massage of the antecubital area after 80 minutes (E). This can usually be achieved also at an earlier time point.
Axial reconstructions and maximum intensity projections (MIP) from the source images of all datasets (3D T2-FS,
mDixon GRE for MRL and combined MRV/MRL) are generated routinely (Fig. 12):
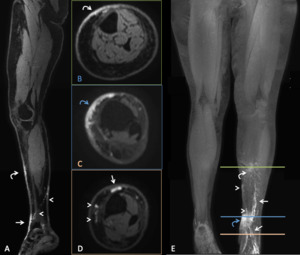
Fig. 12: Lymphatic map with multiplanar reformations of sagittal high resolution 3D mDixon T1 weighted images of left lower extremity obtained 35minutes after interdigital intradermal gadolinium administration of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% (TE 5.7/6.9ms). No venous contamination and complete blood pool supression are observed. There is mild edematous swelling due to lymphatic obstruction in the distal lower leg with distinct lymphatic channels crossing the mortise at 12 o'clock (arrows), 9 o'clock (arrowheads) and with dermal backflow (curved arrows):
A) sagital source image, B)-D) axial, E) 3D MIP reconstruction.
The peripheral-central massage described in the previous section,
however,
serves two purposes for USPIO-enhanced MR lymphangiography:
- To promote migration of interstitially injected gadolinium contrast within the lymphatics centrally (identical to the conventional MRL).
- More importantly: To promote complete equilibrium between intravascular ferumoxytol and the blood pool to minimize the occurrence of hyperintense blood pool signal due to slow flow.
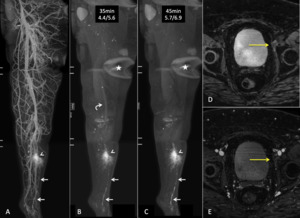
Fig. 13: 56 year-old women who developed moderate lymphoedema of the left lower extremity after hysterectomy, oophorectomy, pelvic lymphnode dissection and radiation of the pelvis:
A) MRV/MRL after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% with intravascular ferumoxytol and short TE pair of 2.8/4.2ms demonstrates patent deep venous system of the extremity and distally obstructed lymphatic channels (arrows) terminating at an area of dermal backflow (arrowheads). Lymphatics are much better seen and distinguishable from veins on modified MRL with higher TEs (B and C) obtained 35min and 45min after injection. Note that complete suppression ob blood pool in this patient is achieved with the longer TE pair of 5.7/6.9ms (multistation MIP of high resolution mDixon T1 weighted GRE images with signal drop artifact most noticeable at the coil end of the superior and mid stack - asterix).
D) Axial mDixon T1 weighted GRE image with long TE pair of 5.7/6.9ms demonstrates contrast pooling of gadolinium in a lymphocele (yellow arrow) 50 minutes after interdigital injection, likely the etiology of distal lower leg edema due to disrupted pelvic lymphatic channels. Gadolinium at the inguinal level confirms adequacy of the delay of the last time point: lymphatic channels between the area of dermal backflow in the lower leg and the pelvis can be therefore excluded. E) MRV/MRL at the same level as D) with TE of 2.8/4.2ms demonstrates patency of the common femoral veins, while the signal of ferumoxytol in the lymphocele is weaker than on the MRL with longer the TE pair.
Comparison of conventional versus USPIO-enhanced MR lymphangiography:
| |
conventional MRL |
USPIO enhanced MRL |
| intravenous infusion of ferumoxytol |
- |
+ |
| intradermal gadolinium injection |
+ |
+ |
| 3D-T2-FS |
+ |
+ |
| 3D-T1-FS: m-FFE Dixon* |
TR=6.2ms
TE1=1.5ms
TE2=2.8ms
FA=20°
|
TR≈TE2+1.7ms
TE1=3.5-8.0ms
TE2≈TE1+1.2ms
FA=20°
|
| intravenous gadolinium injection for MR venogram |
+ |
- |
| volumetic calculation of extremity |
+ |
+ |
*(Philips Ingenia 3T)
Pitfalls and limitations of the USPIO enhanced MR lymphangiography technique:
1.
TE pairs of mDixon T1 weighted sequences must be selected based on the field strength of the scanner and must be chosen such that the fat signal experiences an approximately 180° phase shift between the echoes for the field strength used,
with each echo approximately in- or out of phase. Our experience is limited to 3T, and the longest TE2 was 8.0ms.
If TE pair is chosen too short incomplete venous blood suppression will result ( Fig. 11,
Fig. 13,
Fig. 14 and Fig. 15)
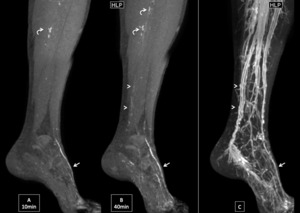
Fig. 14: Insufficient blood pool suppression: A) and B) MRL of left lower extremity with TE 5.7/6.9ms at 10min and 40min after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% demonstrate one dominant lymphatic vessel at the dorsum of the foot (arrow) after lymphovenous anastomosis (LVA) performed above the ankle for lymphatic obstruction.
Focal signal in more superior sections of deep veins is typical for incomplete admixture of ferumoxytol and blood in venous valves (curved arrows). There is also weak contrast enhancement in the posterior tibial veins after 40min (arrowheads), but not after 10min or after 60min (not shown); this finding which was also seen prior to LVA likely reflects the peak time period in which lymphatic gadolinium is shunted into the veins from the site of injection and independent from the lympho-venous anastomosis. The R2* effect of ferumoxytol is not sufficient to suppress the signal intensity of gadolinium. A correction towards a longer TE pair could have been attempted to increase the ferumoxyde effect on blood pool suppression, but would also have resulted in further decrease of gadolinium signal in the lymphatics due to the R2* effect of gadolinium with incresing echo times.
There is however no diagnostic challenge of misinterpretation of the posterior tibial veins for lymphatic vessels due to their typical appearance as paired veins on the MR venogram (C).
2.
TE pairs longer than 7.4ms may show fat-water swap artifacts with the result of gadolinium effacement Fig. 15
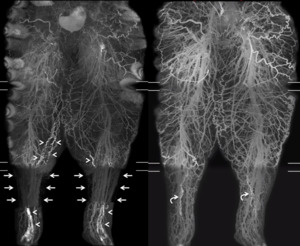
Fig. 15: Fat-water swap artifact: severe bilateral lower extremity lymphoedema with decreased venous flow preventing equilibrium of ferumoxytol and blood leaving the entire blood pool relatively signalintense due to slow flow on MR lymphangiogram (left image). An attempt to mitigate the high blood signal intensity with an increased TE pair in the lower leg segment beyond TE=6.9/8.0ms led to fat-water artifacts (arrows) supressing all vessels including the interstitially injected gadolinium within the abnormally dilated and slightly tortuous lymphatic channels, which are otherwise seen above and below that affected segment (arrowheads).
The lymphatic vessels of this segment are only seen on the MR venogram with a short TE pair (curved arrows on the right image).
Multistation MIP reconstructed from ferumoxytol-enhanced sagittal high resolution mDixon T1 gradient echo images after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% into each extremity.
3.
Within straight vascular segments parallel to the slice select gradient central signal voids may occur in the MRV with short TE pairs.
Depending on the affected vessel this can make the differentiation of this artifact from thrombus,
venous scarring or position-related compression difficult (Fig. 16)

Fig. 16: Flow void on ferumoxytol enhanced MR venogram with short echo time pair: no signal is seen in the brachial vein of the right upper extremity (segment in between long arrows on the left image). Also the distal segments of the deep veins of the forearem are not seen.
Right image demonstrates close up view of the upper arm with thin linear signal at the periphery of the expected brachial vein (arrowheads), representing slow flowing peripheral blood components within the brachial vein, vasa vasorum or the brachial vein or thin accompanying veins.
Multistation MIP of sagittal high resolution mDixon T1 weighted images after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1%).
Advantages of USPIO enhanced MR Lymphangiography
- Highly selective gadolinium contrast-enhanced lymphatic maps with significantly less venous contrast contamination compared to conventional MRL (p<0.001,
Ripley et al.
2017)
- The injection of gadolinium for the purpose of the MR venogram is obsolete since veins are depicted with high signal intensity on T1w GRE pulse sequences using short echo times in the presence of ferumoxytol
Disadvantages of USPIO enhanced MR Lymphangiography
- Requires intravenous administration of ferumoxytol,
which has been reported to cause hypersensitivity reactions including anaphylaxis,
if infused too rapidly*
- Close monitoring is required due to the potential for adverse events such as hypersensitivity
- Signal loss of circulating ferumoxytol observed in straight segments of mainly deep veins parallel to the slice select gradient making the distinction between flow void,
compression and venous thrombus or encasement due to scarring occasionally difficult
- Long echo times may lead to fat-water swap artifacts decreasing conspicuity of gadolinium of ferumoxytol signal
- Higher cost associated with ferumoxytol
* Moderate-to-severe hypersensitivity reactions have been reported in 1.3%.
Slow infusion of ferumoxytol over ≥15min has not shown to cause anaphylactic reactions in a recent study with safety as a secondary study endpoint.
(Adkinson et al.,
2018).


:
A) MRV/MRL (short TE pair) shows veins besides areas of dermal backflow (arrowheads) as a sign of lymphatic obstruction. Dynamic MR lymphangiograms at four different time points (B-E) with increasing TE pairs demonstrate lymphatics more efficiently through signal suppression of blood pool with longer echo times. Note that short segments of signalintense slow or stagnating blood flow with poor admixture of ferumoxytol (curved arrows) could be successfully eliminated with a longer TE pair of 6.2/7.4ms and repeated massage of the antecubital area after 80 minutes (E). This can usually be achieved also at an earlier time point.")
. No venous contamination and complete blood pool supression are observed. There is mild edematous swelling due to lymphatic obstruction in the distal lower leg with distinct lymphatic channels crossing the mortise at 12 o'clock (arrows), 9 o'clock (arrowheads) and with dermal backflow (curved arrows):
A) sagital source image, B)-D) axial, E) 3D MIP reconstruction.")
 MRV/MRL after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% with intravascular ferumoxytol and short TE pair of 2.8/4.2ms demonstrates patent deep venous system of the extremity and distally obstructed lymphatic channels (arrows) terminating at an area of dermal backflow (arrowheads). Lymphatics are much better seen and distinguishable from veins on modified MRL with higher TEs (B and C) obtained 35min and 45min after injection. Note that complete suppression ob blood pool in this patient is achieved with the longer TE pair of 5.7/6.9ms (multistation MIP of high resolution mDixon T1 weighted GRE images with signal drop artifact most noticeable at the coil end of the superior and mid stack - asterix).
D) Axial mDixon T1 weighted GRE image with long TE pair of 5.7/6.9ms demonstrates contrast pooling of gadolinium in a lymphocele (yellow arrow) 50 minutes after interdigital injection, likely the etiology of distal lower leg edema due to disrupted pelvic lymphatic channels. Gadolinium at the inguinal level confirms adequacy of the delay of the last time point: lymphatic channels between the area of dermal backflow in the lower leg and the pelvis can be therefore excluded. E) MRV/MRL at the same level as D) with TE of 2.8/4.2ms demonstrates patency of the common femoral veins, while the signal of ferumoxytol in the lymphocele is weaker than on the MRL with longer the TE pair.")
 and B) MRL of left lower extremity with TE 5.7/6.9ms at 10min and 40min after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% demonstrate one dominant lymphatic vessel at the dorsum of the foot (arrow) after lymphovenous anastomosis (LVA) performed above the ankle for lymphatic obstruction.
Focal signal in more superior sections of deep veins is typical for incomplete admixture of ferumoxytol and blood in venous valves (curved arrows). There is also weak contrast enhancement in the posterior tibial veins after 40min (arrowheads), but not after 10min or after 60min (not shown); this finding which was also seen prior to LVA likely reflects the peak time period in which lymphatic gadolinium is shunted into the veins from the site of injection and independent from the lympho-venous anastomosis. The R2* effect of ferumoxytol is not sufficient to suppress the signal intensity of gadolinium. A correction towards a longer TE pair could have been attempted to increase the ferumoxyde effect on blood pool suppression, but would also have resulted in further decrease of gadolinium signal in the lymphatics due to the R2* effect of gadolinium with incresing echo times.
There is however no diagnostic challenge of misinterpretation of the posterior tibial veins for lymphatic vessels due to their typical appearance as paired veins on the MR venogram (C).")
. An attempt to mitigate the high blood signal intensity with an increased TE pair in the lower leg segment beyond TE=6.9/8.0ms led to fat-water artifacts (arrows) supressing all vessels including the interstitially injected gadolinium within the abnormally dilated and slightly tortuous lymphatic channels, which are otherwise seen above and below that affected segment (arrowheads).
The lymphatic vessels of this segment are only seen on the MR venogram with a short TE pair (curved arrows on the right image).
Multistation MIP reconstructed from ferumoxytol-enhanced sagittal high resolution mDixon T1 gradient echo images after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1% into each extremity.")
. Also the distal segments of the deep veins of the forearem are not seen.
Right image demonstrates close up view of the upper arm with thin linear signal at the periphery of the expected brachial vein (arrowheads), representing slow flowing peripheral blood components within the brachial vein, vasa vasorum or the brachial vein or thin accompanying veins.
Multistation MIP of sagittal high resolution mDixon T1 weighted images after intradermal injection of 2.5cc gadobenate dimeglumine mixed with 2.5cc lidocaine 1%).")