In total,
8 patients (mean age of 55.1 years,
range 33-68) with unusual renal masses were found.
Among these patients,
2 had a histopathologic diagnosis of leiomyoma,
one of cystic nephroma,
one of a mesenchymal neoplasm,
one of metanephric adenoma,
one of focal xanthogranulomatous pyelonephritis,
one of breast metastasis and one of an epidermoid cyst.
Leiomyoma
Leiomyoma is a benign mesenchymal neoplasm originated from smooth muscle cells and in the genitourinary system,
it is more commonly known to affect the bladder.
Renal leiomyomas account for 1.5% of the benign lesions and 0.29% of all treated renal tumors.
It is usually asymptomatic but can produce mass effect,
palpable flank mass,
flank pain or hematuria.
These lesions are more frequently peripheral,
localized in the lower pole and have no side predilection.
At CT scan,
the lesion usually presents as a well-defined mass with no signs of invasion of adjacent parenchyma and demonstrates a high attenuation on precontrast phase.
After contrast media injection,
it shows a progressive enhancement on the later phase.
Larger masses can have heterogeneous enhancement due to hemorrhage and cystic or myxoid degeneration [4–6].
Case 1: Female patient (68 y.o.)
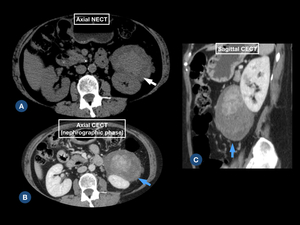
Fig. 1: CT scan shows a (A) heterogeneous, hyperdense peripheral exophytic mass in lower pole of the left kidney (white arrow), (B,C) with mild enhancement on postcontrast phases (blue arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR
Case 2: Female patient (33 y.o.)
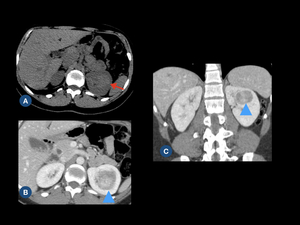
Fig. 2: (A) Nonenhanced CT image shows a homogenous and slightly hyperdense left renal endophytic nodule (red arrow). (B,C) Postcontrast axial and coronal CT images show slight enhancement (blue arrowhead).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR
Cystic nephroma
Multilocular cystic nephroma is a slow growing,
benign renal neoplasm.
It usually presents as an unilateral cystic mass with irregular septa of various thickness.
It is subdivided into cystic nephroma and cystic partially differentiated nephroma depending on the absence or presence of blastemal cells,
respectively.
Multilocular cystic nephroma has a bimodal distribution,
affecting children (mostly boys) and adults between 40-60 years (mostly women).
Possible clinical symptoms in children are painless abdominal mass,
hematuria and urinary tract infection.
In adults,
abdominal pain and hematuria are the most common symptoms,
while hypertension,
painless mass and urinary tract infection are rarer.
At CT,
it is a well-circumscribed,
encapsulated,
multicystic mass with variably enhancing septa and no excretion of contrast into the cystic components.
Cysts content attenuation is similar or slightly higher than that of water.
At MR,
the usual aspect is of a multicystic mass with capsule and septa that are hypointense in all pulse sequences (probably due to fibrous tissue).
The cysts contents are hyperintense on T2-weighted images and have variable intensity on T1-weighted images (presumably because of different concentrations of blood content or protein).
Imaging techniques cannot differentiate multilocular cystic nephroma from malignant multilocular cystic lesions [7-9].
Case 3: Female patient (56 y.o.)
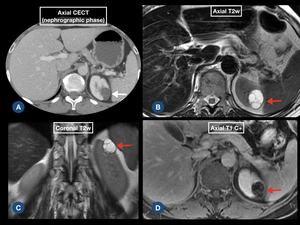
Fig. 3: (A) CECT scan shows a well-circumscribed, encapsulated cystic lesion with slight enhancement in the left kidney (white arrow). (B,C,D) MR images demonstrate thin enhanced septa in the cystic lesion (red arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR
Mesenchymal neoplasm
According to histogenesis and histopathologic findings,
2004 World Health Organization classifies primary renal tumors in adults into the following types: renal cell,
metanephric,
mesenchymal,
mixed mesenchymal and epithelial,
neuroendocrine,
and germ cell tumors.
Mesenchymal neoplasm has vascular,
fibrous,
adipose or other mesenchymal tissue differentiation.
It is classified based on the histologic features and clinical-biologic behavior into a benign or malignant tumor.
Some benign types are angiomyolipoma,
leiomyoma,
hemangioma,
lymphangioma,
juxtaglomerular cell tumor,
renomedullary interstitial cell tumor,
lipoma,
solitary fibrous tumor,
and schwannoma,
while malignant tumors include leiomyosarcoma,
rhabdomyosarcoma,
angiosarcoma,
osteosarcoma,
synovial sarcoma,
fibrosarcoma,
malignant fibrous histiocytoma,
and solitary fibrous tumor.
Radiological appearance is variable and some mesenchymal tumors have characteristic imaging finding and anatomical distribution.
Some cases though remain unclear requiring histological evaluation [10,11].
Case 4: Male patient (62 y.o.)
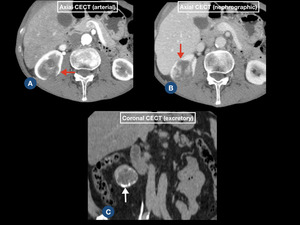
Fig. 4: (A,B,C) CECT scan images demonstrate a heterogeneous, hypovascular right renal mass (red arrows) with peripheral calcifications (white arrow).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR
Metanephric adenoma
Metanephric adenoma is a rare,
benign neoplasm of epithelial cells.
It can present at any age,
but is more common in adults with 50-60 years and has a female predilection.
Possible clinical symptoms include abdominal pain,
hematuria and a palpable mass.
Polycythemia can also be associated.
At CT,
the majority of lesions are solid,
well defined,
isodense on precontrast phase,
enhancing gradually on postcontrast phases.
Sometimes,
the mass can have some hypodense areas due to cystic changes and necrosis.
At MR,
metanephric adenoma findings are limited,
being described as a lesion with low or isosignal intensity on T1 and T2-weighted images.
The main differential diagnosis is renal cell carcinoma,
particularly the papillary subtype that is hypovascular on postcontrast phase [12–14].
Case 5: Female patient (55 y.o.)
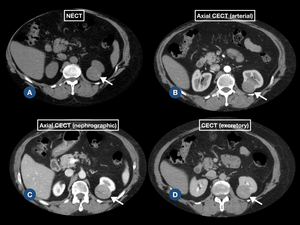
Fig. 5: (A,B,C,D) Axial CT images show a well-defined, hypovascular and homogeneous left renal solid mass (arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR
Focal xanthogranulomatous pyelonephritis
Xanthogranulomatous pyelonephritis is a chronic granulomatous process associated with recurrent bacterial urinary tract infection and is characterized by replacement of normal renal parenchyma with lipid-laden macrophages.
The most common organisms implicated are Proteus mirabilis and Escherichia coli.
Female patients are reported as more affected by this condition and renal pelvic calculi are considered a predisposing factor.
Possible symptoms are fever,
malaise,
flank pain,
hematuria,
palpable mass,
lower tract urinary infection symptoms and weight loss.
This disease usually affects the entire kidney,
while focal involvement is a rare condition,
mimicking a renal neoplasm.
Diffuse form is characterized by a nonfunctioning enlarged kidney,
staghorn calculus in a contracted pelvis,
expansion of calyces and inflammation of perinephric fat.
The focal type is described as a masslike lesion involving the renal cortex without renal pelvic communication and in this form,
the renal stone may not be seen.
At CT and MR,
the lesion may not be distinguished from renal malignancy [15–18].
Case 6: Female patient (62 y.o.)
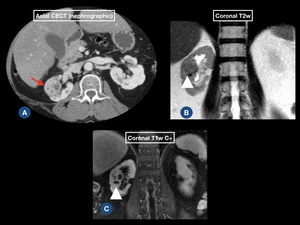
Fig. 6: (A) CT scan demonstrates a heterogeneous, ill-defined mass in the right kidney (red arrow). (B,C) MR images show areas of cystic degeneration / liquefaction into the renal mass (white arrowheads).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR
Breast metastasis
Breast cancer is the most common female malignancy and the majority of cases are not metastatic when diagnosed.
Common sites for metastasis are lung,
bone,
liver,
lymph nodes and skin.
The kidney is a rare location for clinically manifested breast cancer metastasis,
although microscopic metastasis are fairly common at autopsy.
Patient can present with gross hematuria and flank pain or be asymptomatic.
Imaging characteristics are nonspecific.
There are reports of small,
multiple circumscribed rounded masses of relatively low density with poor enhancement and of solitary large mass with an ill-defined margin,
both corresponding to breast metastasis [19–22].
Case 7: Female patient (57 y.o.)
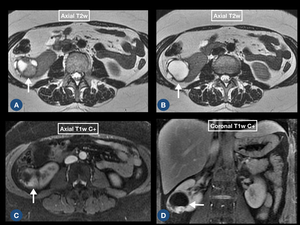
Fig. 7: (A,B,C) MR images demonstrate a heterogeneous, solid-cyst mass in the right kidney (arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR
Epidermoid cyst
Epidermoid cyst is a cyst lined by stratified squamous epithelium with a granular layer and filled with keratinous material.
It is usually located in areas on the skin surface and in the infundibulum of hair follicles.
Renal epidermoid cysts are rare and few cases have been reported.
The most accepted theory for their existence is that they are probably originated from epidermal remnants derived from the Wolffian duct.
Most commonly reported symptoms are flank pain and hematuria.
This disease should be considered when calcified renal masses or well-circumscribed benign calcified cysts are characterized [23,24].
Case 8: Male patient (49 y.o.)
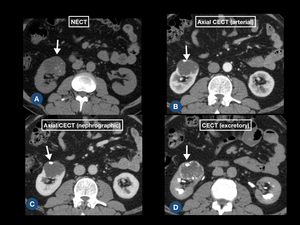
Fig. 8: CT scan demonstrate a well-defined cystic lesion with multiple peripheral calcifications and slight septa enhancement in the right kidney (arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR

 heterogeneous, hyperdense peripheral exophytic mass in lower pole of the left kidney (white arrow), (B,C) with mild enhancement on postcontrast phases (blue arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")
 Nonenhanced CT image shows a homogenous and slightly hyperdense left renal endophytic nodule (red arrow). (B,C) Postcontrast axial and coronal CT images show slight enhancement (blue arrowhead).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")
 CECT scan shows a well-circumscribed, encapsulated cystic lesion with slight enhancement in the left kidney (white arrow). (B,C,D) MR images demonstrate thin enhanced septa in the cystic lesion (red arrows). References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")
 CECT scan images demonstrate a heterogeneous, hypovascular right renal mass (red arrows) with peripheral calcifications (white arrow).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")
 Axial CT images show a well-defined, hypovascular and homogeneous left renal solid mass (arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")
 CT scan demonstrates a heterogeneous, ill-defined mass in the right kidney (red arrow). (B,C) MR images show areas of cystic degeneration / liquefaction into the renal mass (white arrowheads).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")
 MR images demonstrate a heterogeneous, solid-cyst mass in the right kidney (arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")
.
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo - São Paulo/BR")