We reviewed approximately 200 CT scans and 100 MR scans of brain over a period of ~4 years in a tertiary centre and found out the most commonly missed pathologies by the reporting junior radiologists and residents in decreasing order of frequencies were:
- Traumatic (Subtle subarachnoid hemorrhage,
subacute subdural hemorrhage,
non-hemorrhagic contusion,
diffuse axonal injury and fractures particularly at the base of the skull,
nasal bones,
and orbital blow out)
- Ischemic ( hyper acute MCA infarct,
watershed infarcts,
infarcts in brainstem and cerebellum particularly in plain CT,
diffuse hypoxic / ischemic injury ,
cerebral venous thrombosis ,
cervical spinal cord infarct visualised in brain MRI)
- Vascular (small aneurysm,
particularly contra lateral aneurysm in bilateral/multiple aneurysms,
vertebral/ carotid artery dissection,
acute internal carotid artery thrombosis)
- Neoplastic (glomus jugulare tumor,
clival/ convexity meningioma ,
small vestibular schwannoma,
trigeminal schwannoma,
small tectal plate lipoma).
- Infective/Inflammatory (meningitis,
skull base osteomyelitis,
small granulomas particularly extra-cranial neurocysticercosis).
TRAUMATIC PATHOLOGIES
Case 1: 45 Years old male with history of road traffic accident
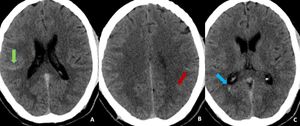
Fig. 1: Findings: NCCT axial images of brain demonstrate subtle linear hyperdensity in the right (green arrow in A) and left parietal sulci (red arrow in B) suggestive of acute subarachnoid haemorrhage(SAH). Minimal intraventricular hemorrhage also seen in the right occipital horn (blue arrow in C).
Diagnosis: Acute subarachnoid and intraventricular hemorrhage
Missed finding /error: Subtle left parietal subarachnoid hemorrhage and intraventricular hemorrhage were missed by reporting junior radiologist.
Learning point: Appropriate windowing can assist in the identification of subtle acute SAH.
Case 2: 63 Year old male with history of fall 5 days back and persistent headache
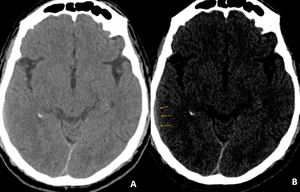
Fig. 2: Axial CT image of brain demonstrate small isodense subacute subdural hemorrhage over right temporal convexity which can be missed by an untrained eye (A). On subdural window hemorrhage can be better appreciated (orange arrows in B).
Diagnosis: Subacute subdural hemorrhage
Learning point: Using multiple window settings is very important in the case of trauma.
Medial shift of the grey / white matter interface can also help in the diagnosis of subacute subdural hemorrhage on CT images.
Case 3: 25 Year old male with history of road traffic accident 5 hours back
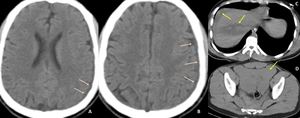
Fig. 3: Non-contrast CT images (A & B) of brain demonstrates isodense subdural collection over the left parietal lobe. Non contrast axial images of abdomen demonstrates liver laceration ( yellow arrow in C) and gross hemoperitoneum. This was case of acute isodense subdural hemorrhage.
Diagnosis: Isodense acute subdural hemorrhage
Learning point: In case of trauma with severe blood loss,
acute SDH can be isodense which is difficult to diagnose on CT.
Careful observation of dural margins and medial shift of the grey / white matter interface can also help in the diagnosis of isodense subdural hemorrhage on CT images.
Case 4: 24 Years old male with history of road traffic accident
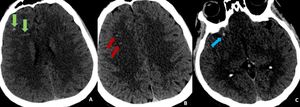
Fig. 4: Findings: Non-contract CT axial images of brain demonstrate multiple punctate hemorrhagic contusions in right frontal lobe predominantly at grey white matter junction suggestive of diffuse axonal injury. At times, CT findings may be subtle and can be easily missed.
Diagnosis: Diffuse axonal injury
Learning point: Appropriate windowing can assist in the identification of punctate haemorrhagic contusions.
Case 5: 25 years old male with history of road traffic accident
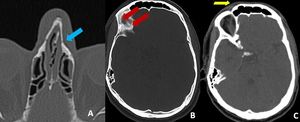
Fig. 5: Axial bone window CT image of head shows subtle left nasal bone fracture (blue arrow in A) and thin linear lucent line in the right supra orbital margin extending along the orbital roof suggestive of fracture (red arrows in B). Subtle superficial soft tissue swelling seen over right orbit (yellow arrow in C).
Diagnosis: Nasal bone and orbital fractures
Missed finding /error: Both fractures were missed by reporting junior radiologist.
Learning point: Soft tissue swelling or air foci may be the clue to identify the undisplaced subtle fractures particularly in the skull base and orbits.
Systematic review of facial and skull base bones using a structured template check list can help in not missing the fractures.
Case 6: 32 year old male with history of road traffic accident
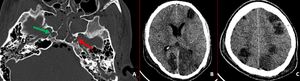
Fig. 6: Axial bone window CT image demonstrates comminuted fracture of left carotid canal (red arrow in A) and mildly displaced fracture of lateral wall of right carotid canal (green arrow in A). Also there are longitudinal fractures of bilateral temporal bones with hemomastoid. Follow up non-contrast CT brain (performed after 3 days) demonstrates multiple varying sized hypo dense areas in bilateral cerebral hemispheres suggestive of infarcts.
Diagnosis: Carotid canal fractures
Missed finding / Error: Right carotid canal fracture was not mentioned by reporting radiologist.
Learning point: “Satisfaction of search” is one of common reasons for missing the findings.
Systematic review of facial and skull base bones using a structured template check list can help in not missing the fractures.
Other fractures that can be missed are:
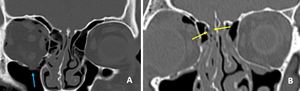
Fig. 7: Coronal CT images showing fracture of right orbital floor (blue arrow in A) and fracture in right cribriform plate (yellow arrows in B).
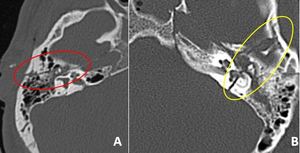
Fig. 8: Axial CT images in bone window showing longitudinal fracture of right temporal bone (A) and transverse fracture of left temporal bone(B).
ISCHEMIC PATHOLOGIES
Case 7: 55 year old female with sudden onset of right sided weakness
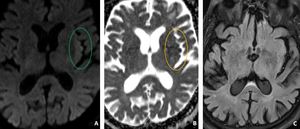
Fig. 9: Axial MR images of brain showing subtle hyperintensity in the left insular cortex on DWI image (A) with corresponding hypointensity on ADC image (B) suggesting diffusion restriction and suggestive of hyper acute left MCA territory infarct. Corresponding FLAIR image (C) demonstrates no abnormality in left insular cortex (Normal looking !).
Diagnosis: Left MCA territory infarct
Learning point: Diffusion restriction in cortex can be very subtle and often difficult to differentiate from the artifacts.
ADC image can help in differentiating.
Case 8: 48 year old male with sudden onset of right sided weakness and sensory loss
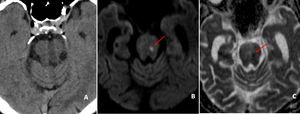
Fig. 10: DWI/ADC axial images of brain showing punctate diffusion restricting focus in mid brain on left side (red arrows in B and C)suggestive of infarct. Corresponding CT image demonstrates no abnormality (A, Normal looking !)
Diagnosis: Acute brain stem infarct
Teaching point: CT images may not demonstrate any abnormality in brain stem in case of acute infarction.
In appropriate clinical scenario performing diffusion MRI is very important.
Case 9: 32 year old female with history of sudden onset of vertigo since 6 hours.
Her brain CT scan was negative.
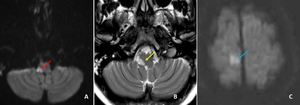
Fig. 11: Axial MR images of brain at the level of medulla showing small hyperintense focus in the right lateral portion of medulla on DWI (red arrow in A) and T2w (yellow arrow in B) images, suggestive of lateral medullary infarct (ADC image not shown).
Axial DWI image of brain demonstrates small acute infarct ( blue arrow in C) demonstrates small acute infarct in the para-sagittal portion of right frontal lobe (This finding was missed by reporting resident).
Diagnosis: Acute right lateral medullary and right frontal lobe infarcts
Learning point: Brain stem being an important blind spot,
small lateral medullary infarcts are prone to be missed by an inexperienced observer.
One should look for all the slices of diffusion to avoid false negative result (particularly upper most and lower most slices!!).
Case 10: 45 years old female with sudden onset right hemiparesis and slurring of speech
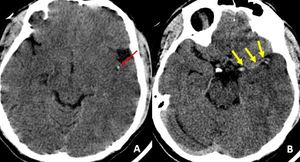
Fig. 12: Axial non-contrast CT ( A) demonstrate hyper dense left MCA (red arrow in A: MCA dot sign and yellow arrows in B: Dense MCA sign) suggestive of thrombosis. It was missed by reporting junior radiologist at the time of initial presentation. Large MCA territory infarct was seen on MRI (Not shown).
Case 11: 29 year male presented with history of sudden collapse at work place.

Fig. 13: Axial noncontrast CT image of brain shows loss of definition of the gray-white matter interface in the lateral margin of the left insular cortex (“Loss of insular ribbon") suggestive of hyper acute infarct. Note to be made of normal definition of gray –white interface in right insular cortex.
Missed finding/Error : This finding was overlooked by reporting radiologist,
probably due to viewing the images with inappropriate window settings.
Learning point: Look for the classical but subtle CT signs of acute infarction (like MCA dot sign,
loss of insular ribbon and disappearing basal ganglia sign) with appropriate window settings
Disappearing basal ganglia sign:
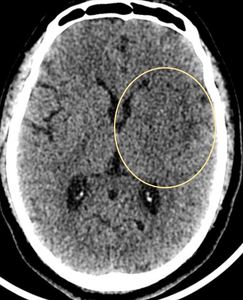
Fig. 14: CT axial image of brain demonstrate loss of delineation of the left basal ganglia suggestive of acute MCA territory infarct.
References: Case courtesy of Dr Prashant Mudgal, Radiopaedia.org. From the case rID: 35604
Case 12: 45 year male presented with history of sudden right sided weakness
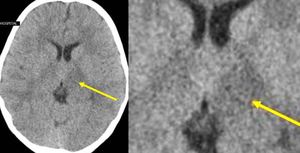
Fig. 15: Axial CT image of brain at the level of basal ganglia demonstrate mild focal hypodensity in the left thalamus and posterior limb of internal capsule suggestive of acute infarct.
Missed finding/Error: Left thalamus and posterior limb internal capsule infarct not mentioned by reporting radiologist.
Learning point: Review every CT brain on a high contrast window to exclude infarcts
Case 13: 72 Year old male with history of sudden onset of vomiting followed by unconsciousness
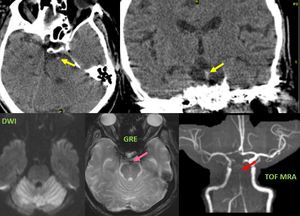
Fig. 16: Axial and coronal non-contract CT images of brain demonstrate subtle hyperdensity in the basilar artery.
MRI performed after 2 hours demonstrate large acute infarct in the bilateral cerebellar hemispheres (C), blooming in the basilar artery on GRE image (pink arrow in D) and loss of flow related intensity in distal portion of basilar artery (red arrow in E) on TOF MRA images.
Diagnosis: Basilar artery thrombosis
Missed finding/Error: Basilar artery hyperdensity was missed on initial CT images.
Learning point: Basilar artery and vertebral artery thrombosis may be subtle on CT images.
Careful systematic review of all the vessels is very important to avoid false negative report.
VASCULAR
Case 14: 65 Years male with history of sudden onset of vertigo and ataxia
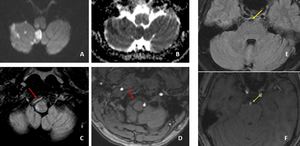
Fig. 17: Areas of diffusion restriction in right cerebellar hemisphere, right middle cerebellar peduncle, right side of medulla and left side of pons (A and B).FLAIR image demonstrate loss of flow void in the right V2 segment of right vertebral artery (red arrow in C). V2 segment of right vertebral artery in not seen on TOF MRA image (red arrow in D).
Linear hyperintensity seen within the basilar artery on FLAIR image (yellow arrow in E) and linear filling defect within the basilar artery on TOF MRA image (green arrow in F), suggestive of basilar artery dissection.
Diagnosis: Basilar artery dissection
Missed finding / Error: Basilar artery dissection was not mentioned by reporting radiologist.
Teaching point: Always should try to identify the cause for infarction.
At times arterial dissections can be subtle appearing as linear filling defects on TOF MRA images and linear hyperintensities traversing within the lumen on FLAIR images.
Case 15: 43 Year old male patient with history of right sided weakness and reduced GCS
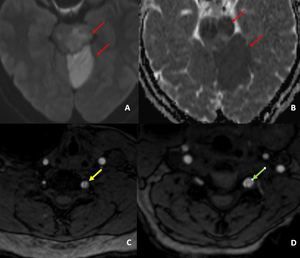
Fig. 18: DWI/ ADC images demonstrates diffusion restriction in left cerebral peduncles, midbrain, pons and left superior cerebellar hemisphere (red arrows in A and B) suggestive of acute infarcts.
TOF MRA images demonstrate linear filling defects in V1 segment of left vertebral artery ( yellow arrow in C), suggestive of dissection and eccentric rounded filling defect in V1 segment of left vertebral artery (green arrow in D) suggestive of thrombosis.
Diagnosis: Vertebral artery dissection
Missed finding / Error: Left vertebral thrombosis was reported; dissection was not mentioned.
Learning point: Dissection and thrombosis can co-exist and identifying dissection can potentially alters the management.
Case 16: 35 Year old female patient with history of headache
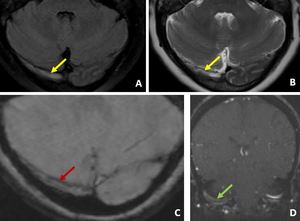
Fig. 19: FLAIR and T2W images of brain demonstrate loss of flow void in right transverse sinus (yellow arrows in A and B). GRE image of brain demonstrating blooming lines in right transverse sinus (red arrow in C). TOF MRV image demonstrate loss of flow related enhancement (green arrow in D). Features suggestive of dural venous thrombosis. Brain parenchyma showed no abnormality.
Diagnosis: Dural venous thrombosis
Missed finding/Error: Thrombosis was not diagnosed on FLAIR / T2W / GRE images.
Learning point: Absence of normal flow void should prompt for the obtaining TOF MRV images
Case 17: 66 Year old male presented with altered sensorium
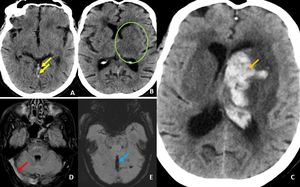
Fig. 20: Initial axial CT images of brain demonstrates ill defined hypodensity in the left basal ganglia and thalamus ( green ring in B) . There is moderate hyperdensity in the internal cerebral veins ( yellow arrows in A) , which is suspicious for thrombosis.
Follow up (after 24 hours ) axial CT image (demonstrates large left basal ganglia infarct with hemorrhagic transformation (orange arrow in C). Axial MRI images acquired after 12 hours of the initial CT demonstrates loss of flow void in internal cerebral vein, straight sinus and bilateral transverse sinuses on FLAIR sequences (red arrow in D). These veins also demonstrate blooming on GRE images (blue arrow in E). Features are suggestive of dural venous thrombosis.
Diagnosis: Dural venous thrombosis
Missed finding / Error: Hyperdensity in the internal cerebral veins was overlooked in the initial CT images.
Learning point: In the presence of acute infarcts one should look both arterial or venous thrombosis.
Early detection of venous thrombosis can influence the management.
NEOPLASMS
Case 18: 30 Years female with history of right sided headache since 1 month
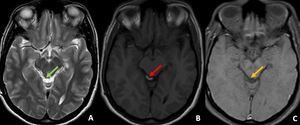
Fig. 21: Small T1w hyperintense lesion arising from the right tectal plate which is supressing on T1w fat suppression sequence, suggestive of tectal lipoma. On close observation T2w hyperintense lesion seen in the same location.
Diagnosis: Tectal plate lipoma
Missed finding/Error: Lesion was not reported by junior reporting radiologist
Learning point: Small lipomas can be confidently identified only on T1w images as bright objects
Case 19: 75 years old female with history of left sided tinnitus

Fig. 22: Axial and coronal CT images in bone window demonstrate destructive changes around the left jugular canal (red arrows in A and B). Post contrast CT axial image demonstrates markedly enhancing mass (green arrow in C) in the left jugular canal suggestive of paraganglioma like glomus jugulare
Diagnosis: Glomus jugulare
Learning point: Skull base erosions may be subtle.
Systematic review of the skull base structures can help in avoiding the false negative report.
Case 20: 15 year old girl with history of headache particularly in the right frontal region since last 6 months increasing in frequency in last 2 months
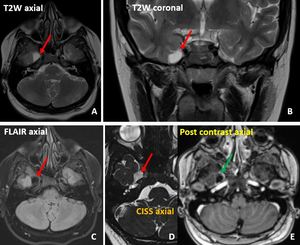
Fig. 23: Small extra-axial cystic lesion in the inferior aspect of the right medial temporal lobe showing central fluid intensity (red arrows in A, B, C, D) and mild peripheral enhancement (green arrow in E). This was a case of Trigeminal cystic Schwannoma. Such lesions can be potentially missed.
Diagnosis: Right trigeminal nerve cystic schwannoma
Case 21: 35 year female with history of left facial pain and numbness since 2 months
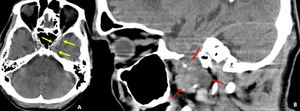
Fig. 24: Axial and parasagittal CT images demonstrates well-delineated mildly hypodense mass lesion in the left Meckel's cave expanding the foramen ovale and extending to the masticator space. This was a case of left trigeminal nerve schwannoma.
Lesion is subtle on axial images (yellow arrows in A) but very much evident on parasagittal images (red arrows in B). This lesion was not mentioned by reporting radiologist.
Diagnosis: Left trigeminal nerve schwannoma
Learning point: Systematic review of the skull base structures and foramena can help in avoiding the false negative finding
Case 22: 25 year female with history of headache
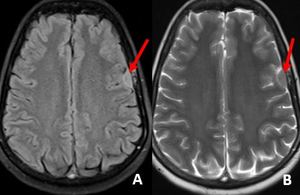
Fig. 25: Small FLAIR and T2W isointense extra axial mass (red arrows in A and B) over the left frontal lobe suggestive of small convexity meningioma. Such lesions can be missed on noncontrast studies.
Diagnosis: Convexity meningioma
Case 23: 50 years old male with headache and right sided hearing loss
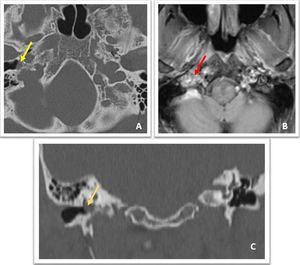
Fig. 27: Non contrast axial and coronal CT images demonstrate small soft tissue dense lesion in the right middle ear cavity with subtle erosions of adjacent antero-lateral margin of jugular foramen (yellow arrow in A and orange arrow in C). Contrast enhanced axial T1w MR image demonstrates heterogeneous marked enhancement of the lesion (red arrow in B). Features are suggestive of glomus tympanicum.
Diagnosis: Right glomus tympanicum
Missed finding / Error: Although mass was mentioned in the CT image,
bony erosions were not mentioned in the report.
Learning point: Viewing the lesion in bony window in all the planes can depict subtle erosions which altogether changes the diagnosis.
Case 24: 35 Year old female with history of right sided reduced hearing
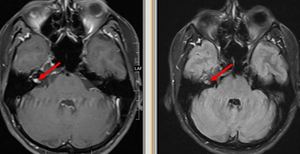
Fig. 28: Axial post contrast T1w and post contrast FLAIR images shows small soft tissue enhancing mass encasing the distal cisternal portion of right vesibulocochlear - facial nerve complex within the internal auditory canal. This was a case of vestibular schwannoma. Such small cranial nerve lesions can be easily missed.
Diagnosis: Vestibular schwannoma
INFECTIVE/INFLAMMATORY PATHOLOGIES
Case 25: Known case of neurocysticercosis

Fig. 26: Noncontract axial CT of brain showing small cyst with central hyperdensity (scolex) in the left lateral rectus muscle in a known case of disseminated neurocysticercosis. This lesion was missed by the reporting
radiologist.
Case 26: 60 Year female underwent left sided ear surgery 6 months back; now came with history of neck pain
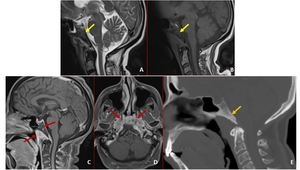
Fig. 29: A and B:Initial sagittal MRI demonstrates abnormal T1w and T2w hypo intense signal changes in the clivus (yellow arrows in A and B). These findings are not reported by the reporting radiologist. The pain was attributed to cervical spine degenerative changes.
C-E: Patient came after 2 months with persistent symptoms of neck pain, low grade fever and right facial nerve palsy. T1w post contrast MRI sagittal and axial images demonstrate heterogeneously enhancing abnormal soft tissue in pharyngeal mucosal space adjacent to clivus (red arrows in C and D). There is heterogeneous enhancement of the clivus in association with replacement of normal hyperintense fatty marrow, features are consistent with skull base osteomyelitis. Corresponding sagittal CT image demonstrates patchy sclerosis in the clivus (orange arrow in E).
Diagnosis: Skull base osteomyelitis
Missed finding / Error: Abnormal signal changes in the clivus was not mentioned in the initial MRI by the reporting radiologist.
Learning point: Hypointense fatty marrow of clivus on T1w images suggest marrow replacement.
Case 27: 42 Year female patient with history of pain in the bilateral orbital region with no vision loss
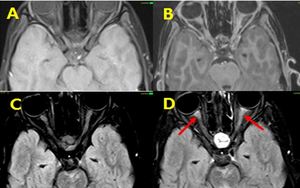
Fig. 30: Unenhanced T1W axial and FLAIR images show normal appearing bilateral optic nerves ( A and C). There is mild enhancement of optic nerves on post contrast T1w images which better appreciated on post contrast FLAIR images ( red arrows in D). This was case of Neuromyelitis optica.
Diagnosis: Neuromyelitis optica
Learning point: Cranial nerve abnormalities like neuritis and spread of the malignancy are better seen on post contrast FLAIR sequences compared to post contrast T1w images.
Case 28: 32 year old female with history of headache
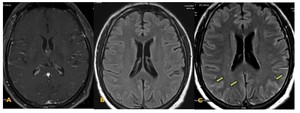
Fig. 31: Post contrast T1W axial image (A) shows normal appearing cortical vessels with no obvious evidence of abnormal meningeal enhancement. Unenhanced axial FLAIR image showing no abnormality (B). Post contrast T2W FLAIR axial image showing abnormal leptomeningeal enhancement in the form of marked sulcal hyper intensity in bilateral parietal and occipital lobes. This was a case of viral meningitis.
Diagnosis: Viral meningitis
Learning point: Mild – moderate leptomeningeal enhancement may not be detected on post contrast T1w images.
Even subtle leptomeningeal enhancement can be readily detected on post contrast FLAIR sequences.
This sequence should be considered in suspected case of meningeal pathologies.
Case 29: 41 Year old female with history of numbness of over left half of the face since 3 days with mild headache
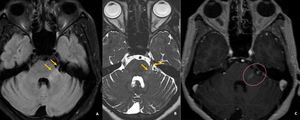
Fig. 32: Axial MR images of brain demonstrate subtle hyperintensity in the cisternal portion of the left trigeminal nerve and its nucleus on FLAIR and CISS images (orange arrows in A and B). Post contrast T1w image demonstrates mild enhancement of the nerve. Features suggestive of trigeminal neuritis.
Diagnosis: Trigeminal neuritis
Learning point: Cranial nerves are one of the important blind spots.
Systematic anatomical review of cranial nerves can avoid the errors.
Case 30: 60 Year old male patient with history of fever,
chills and headache,
visual blurring
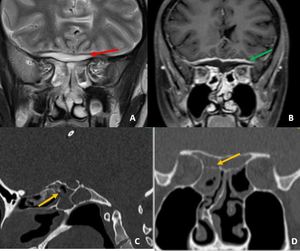
Fig. 40: Coronal T2w image of the brain demonstrates epidural collection along the anterior skull base adjacent to sphenoid sinuses. Diffuse mucosal thickening seen in sphenoid sinuses. Postcontrast T1w image demonstrates thick dural enhancement (green arrow in B) adjacent to the collection. Sagittal and coronal CT images of demonstrates bony erosions along the walls of sphenoid sinuses. Features of suggestive of complicated sinusitis with anterior skull base epidural abscess.
Diagnosis: Skull base osteomyelitis
Learning point: In cases of sinusitis,
always one should look for the features of complications,
particularly of skull base and intracranial complications
OTHER PATHOLOGIES
Case 31: 21 years old female with seizure,
cardiac arrest and post resuscitation status
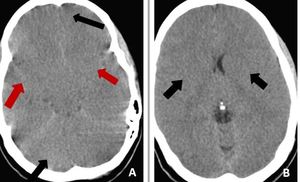
Fig. 33: Non-contrast CT scan of brain on axial section in brain window reformation (A & B) demonstrate diffuse effacement of sulcal spaces including bilateral sylvian fissures (red arrows) and loss of gray-
white matter interface in bilateral fronto temporal lobes , cerebellum [black arrows in (A)] and bilateral basal ganglia [black arrows in (B)]–these features are suggestive of diffuse cerebral edema from hypoxic/anoxic injury to the brain.
Diagnosis: Diffuse cerebral edema
Missed finding /error: Study was reported as normal by the reporting junior radiologist.
Learning point: Effacement of Sylvain fissures and cerebellar sulcal spaces are the main clues for diagnosis.
Case 32: 24 year-old postpartum woman with history of orthostatic hypotension.
Epidural analgesia was given during delivery
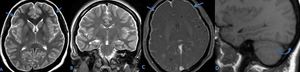
Fig. 34: (A and B) Axial and coronal T2w MR image shows bilateral subdural collections (arrows).
(C) Axial post GD T1w MR image shows diffuse dural enhancement (arrows).
(D) Sagittal non contrast T1w image shows venous distension sign (curved arrow) with inferior convexity of dominant right transverse sinus. Features are suggestive of intracranial hypotension. These findings are often subtle and may be missed,
Diagnosis: Intracranial hypotension
Learning point: One should look for various qualitative and quantitative parameters to diagnose intracranial hypotension.
Case 33: 28 Year old female patient with history of headache since 4 days
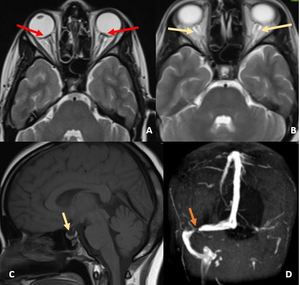
Fig. 35: Axial T2w images of brain at the level of orbits demonstrate prominent bilateral peri-optic CSF spaces (red arrows in A) and flattening of the posterior sclera (arrows in B). T1w sagittal image demonstrates partial empty sella (C) and MRV image demonstrates focal stenosis of right distal transverse sinus. Left transverse and sigmoid sinuses are hypoplastic. Features are suggestive of intracranial hypertension.
Diagnosis: Intracranial hypertension
Learning point: Sella and optic nerves are important review areas in the brain imaging.
Features of intracranial hypertension can be subtle and can be missed.
Case 34: 26-year-old postpartum woman who presented with diabetes insipidus
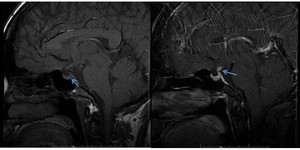
Fig. 36: Sagittal non-enhanced T1w MR image shows loss of normal posterior pituitary bright spot (blue arrow in A). Sagittal post contrast T1w MR image shows enhancement of the thickened infundibulum (blue arrow in B). Features are suggestive of lymphocytic infundibulo-neurohypophysitis. Often such a finding can be subtle and missed.
Diagnosis: Lymphocytic infundibulo-neurohypophysitis
Learning point: Sella is one the important blind spot in MR or CT imaging.
Careful review of pre and post contrast sagittal images is required to avoid false negative results.
Case 35: 35-year old postpartum woman who presented with severe headache and hypertension
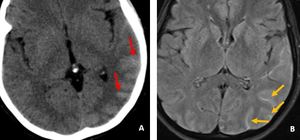
Fig. 37: Axial head CT image shows a subtle hyperdensity in the left temporo-pareital sulci (red arrows in A) . Axial FLAIR MR image shows a sulcal hyperintensity (orange arrows in B) in the left parieto-occipital sulci, consistent with Nonaneurysmal SAH. This was a case of Postpartum cerebral angiopathy.
Diagnosis: Postpartum cerebral angiopathy
Learning point: Focally distributed non-aneurysmal SAH can be easily overlooked on CT images.
One should carefully look at the sulcal spaces (blind spot) on FLAIR images to avoid false negative result.
Case 36: 64-year old male with history of memory loss – 1 day.
No neurological or congestive symptoms
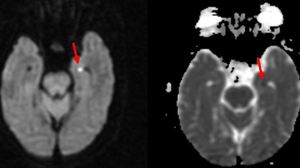
Fig. 38: Axial DWI / ADC images demonstrates small punctate diffusion restricting focus on the lateral margin of left hippocampal gyrus abutting the temporal horn (red arrows in A and B). Rest of the sequences showed no significant abnormality other than mild chronic small vessel ischemic changes(Not shown). Features are suggestive of Transient global amnesia.
Diagnosis: Transient global amnesia
Missed finding / Error: Punctate diffusion restricting focus is not mentioned by reporting junior radiologist.
Learning point: One should aware of this condition and classical location of diffusion restriction.
Case 37: 28 Year old female patient with history of headache since 2 years on and off
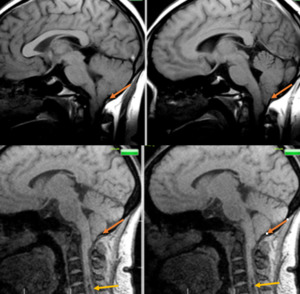
Fig. 39: Sagittal T1w sections of brain demonstrate herniation of cerebral tonsils through the foramen magnum (dark orange arrows) and there is syrinx in the cervical cord at the level of C5 and C6 vertebral levels (light orange arrows. Features are suggestive of Chiari 1 malformation with syrinx. This case was reported as normal study by a junior radiologist
Diagnosis: Chiari 1 malformation with syrinx
Learning point:Craniovertebral junction (CVJ) anomalies,
caudal descent of cerebellar tonsils and cervical spine / cord are often missed by inexperienced radiologists.
Inclusion of CVJ and cervical spine in the review checklist can help in avoiding false negative reports


 and left parietal sulci (red arrow in B) suggestive of acute subarachnoid haemorrhage(SAH). Minimal intraventricular hemorrhage also seen in the right occipital horn (blue arrow in C).")
. On subdural window hemorrhage can be better appreciated (orange arrows in B).")
 of brain demonstrates isodense subdural collection over the left parietal lobe. Non contrast axial images of abdomen demonstrates liver laceration ( yellow arrow in C) and gross hemoperitoneum. This was case of acute isodense subdural hemorrhage.")

 and thin linear lucent line in the right supra orbital margin extending along the orbital roof suggestive of fracture (red arrows in B). Subtle superficial soft tissue swelling seen over right orbit (yellow arrow in C).")
 and mildly displaced fracture of lateral wall of right carotid canal (green arrow in A). Also there are longitudinal fractures of bilateral temporal bones with hemomastoid. Follow up non-contrast CT brain (performed after 3 days) demonstrates multiple varying sized hypo dense areas in bilateral cerebral hemispheres suggestive of infarcts.")
 and fracture in right cribriform plate (yellow arrows in B).")
 and transverse fracture of left temporal bone(B).")
 with corresponding hypointensity on ADC image (B) suggesting diffusion restriction and suggestive of hyper acute left MCA territory infarct. Corresponding FLAIR image (C) demonstrates no abnormality in left insular cortex (Normal looking !).")
suggestive of infarct. Corresponding CT image demonstrates no abnormality (A, Normal looking !)")
 and T2w (yellow arrow in B) images, suggestive of lateral medullary infarct (ADC image not shown).
Axial DWI image of brain demonstrates small acute infarct ( blue arrow in C) demonstrates small acute infarct in the para-sagittal portion of right frontal lobe (This finding was missed by reporting resident).")
 demonstrate hyper dense left MCA (red arrow in A: MCA dot sign and yellow arrows in B: Dense MCA sign) suggestive of thrombosis. It was missed by reporting junior radiologist at the time of initial presentation. Large MCA territory infarct was seen on MRI (Not shown).")
 suggestive of hyper acute infarct. Note to be made of normal definition of gray –white interface in right insular cortex.")


, blooming in the basilar artery on GRE image (pink arrow in D) and loss of flow related intensity in distal portion of basilar artery (red arrow in E) on TOF MRA images.")
.FLAIR image demonstrate loss of flow void in the right V2 segment of right vertebral artery (red arrow in C). V2 segment of right vertebral artery in not seen on TOF MRA image (red arrow in D).
Linear hyperintensity seen within the basilar artery on FLAIR image (yellow arrow in E) and linear filling defect within the basilar artery on TOF MRA image (green arrow in F), suggestive of basilar artery dissection.")
 suggestive of acute infarcts.
TOF MRA images demonstrate linear filling defects in V1 segment of left vertebral artery ( yellow arrow in C), suggestive of dissection and eccentric rounded filling defect in V1 segment of left vertebral artery (green arrow in D) suggestive of thrombosis.")
. GRE image of brain demonstrating blooming lines in right transverse sinus (red arrow in C). TOF MRV image demonstrate loss of flow related enhancement (green arrow in D). Features suggestive of dural venous thrombosis. Brain parenchyma showed no abnormality.")
 . There is moderate hyperdensity in the internal cerebral veins ( yellow arrows in A) , which is suspicious for thrombosis.
Follow up (after 24 hours ) axial CT image (demonstrates large left basal ganglia infarct with hemorrhagic transformation (orange arrow in C). Axial MRI images acquired after 12 hours of the initial CT demonstrates loss of flow void in internal cerebral vein, straight sinus and bilateral transverse sinuses on FLAIR sequences (red arrow in D). These veins also demonstrate blooming on GRE images (blue arrow in E). Features are suggestive of dural venous thrombosis.")

. Post contrast CT axial image demonstrates markedly enhancing mass (green arrow in C) in the left jugular canal suggestive of paraganglioma like glomus jugulare")
 and mild peripheral enhancement (green arrow in E). This was a case of Trigeminal cystic Schwannoma. Such lesions can be potentially missed.")
 but very much evident on parasagittal images (red arrows in B). This lesion was not mentioned by reporting radiologist.")
 over the left frontal lobe suggestive of small convexity meningioma. Such lesions can be missed on noncontrast studies.")
 in the left lateral rectus muscle in a known case of disseminated neurocysticercosis. This lesion was missed by the reporting
radiologist.")
. Contrast enhanced axial T1w MR image demonstrates heterogeneous marked enhancement of the lesion (red arrow in B). Features are suggestive of glomus tympanicum.")

. These findings are not reported by the reporting radiologist. The pain was attributed to cervical spine degenerative changes.
C-E: Patient came after 2 months with persistent symptoms of neck pain, low grade fever and right facial nerve palsy. T1w post contrast MRI sagittal and axial images demonstrate heterogeneously enhancing abnormal soft tissue in pharyngeal mucosal space adjacent to clivus (red arrows in C and D). There is heterogeneous enhancement of the clivus in association with replacement of normal hyperintense fatty marrow, features are consistent with skull base osteomyelitis. Corresponding sagittal CT image demonstrates patchy sclerosis in the clivus (orange arrow in E).")
. There is mild enhancement of optic nerves on post contrast T1w images which better appreciated on post contrast FLAIR images ( red arrows in D). This was case of Neuromyelitis optica.")
 shows normal appearing cortical vessels with no obvious evidence of abnormal meningeal enhancement. Unenhanced axial FLAIR image showing no abnormality (B). Post contrast T2W FLAIR axial image showing abnormal leptomeningeal enhancement in the form of marked sulcal hyper intensity in bilateral parietal and occipital lobes. This was a case of viral meningitis.")
. Post contrast T1w image demonstrates mild enhancement of the nerve. Features suggestive of trigeminal neuritis.")
 demonstrate diffuse effacement of sulcal spaces including bilateral sylvian fissures (red arrows) and loss of gray-
white matter interface in bilateral fronto temporal lobes , cerebellum [black arrows in (A)] and bilateral basal ganglia [black arrows in (B)]–these features are suggestive of diffuse cerebral edema from hypoxic/anoxic injury to the brain.")
 Axial and coronal T2w MR image shows bilateral subdural collections (arrows).
(C) Axial post GD T1w MR image shows diffuse dural enhancement (arrows).
(D) Sagittal non contrast T1w image shows venous distension sign (curved arrow) with inferior convexity of dominant right transverse sinus. Features are suggestive of intracranial hypotension. These findings are often subtle and may be missed,")
 and flattening of the posterior sclera (arrows in B). T1w sagittal image demonstrates partial empty sella (C) and MRV image demonstrates focal stenosis of right distal transverse sinus. Left transverse and sigmoid sinuses are hypoplastic. Features are suggestive of intracranial hypertension.")
. Sagittal post contrast T1w MR image shows enhancement of the thickened infundibulum (blue arrow in B). Features are suggestive of lymphocytic infundibulo-neurohypophysitis. Often such a finding can be subtle and missed.")
 . Axial FLAIR MR image shows a sulcal hyperintensity (orange arrows in B) in the left parieto-occipital sulci, consistent with Nonaneurysmal SAH. This was a case of Postpartum cerebral angiopathy.")
. Rest of the sequences showed no significant abnormality other than mild chronic small vessel ischemic changes(Not shown). Features are suggestive of Transient global amnesia.")
 and there is syrinx in the cervical cord at the level of C5 and C6 vertebral levels (light orange arrows. Features are suggestive of Chiari 1 malformation with syrinx. This case was reported as normal study by a junior radiologist")
 adjacent to the collection. Sagittal and coronal CT images of demonstrates bony erosions along the walls of sphenoid sinuses. Features of suggestive of complicated sinusitis with anterior skull base epidural abscess.")