Imaging Specifications
Field strength
- MR Neurography should be performed either at 3T or 1.5T MRI systems.
- 3T systems are preferred because they provide greater signal-to-noise ratio (SNR),
which can result in higher resolution images and/or faster acquisition times.
- 1.5T systems should be used when scanning patients with metallic implants to reduce susceptibility artifacts.
Imaging plane
- Traditional protocols include all three imaging planes (axial,
coronal,
sagittal).
- Coronal is the most important plane because it can depict all nerves together and demonstrates their longitudinal extent.
- Sagittal plane should be used to assess the relationship of pathology to the plexus components and subclavian and axillary arteries.
Slice positioning
- Coronal: Slices should be parallel to the line joining the right and left transverse process of the cervical spine in the axial plane and parallel to the spinal cord in the sagittal plane.
Wrong angulation in the sagittal plane may lead to insufficient imaging of the brachial plexus (fig.
4) Cover the entire brachial plexus from the cervical vertebrae to the spinous processes.
Field-of-view (FOV) should be big enough to cover the whole brachial plexus from the right to left shoulder (typically 32-38 cm).
- Axial: Slices should be perpendicular to the spinal cord in the sagittal and coronal plane.
Cover the entire brachial plexus from the C3 vertebra to the T4 vertebra.
Field-of-view (FOV) should be big enough to cover the whole brachial plexus from the right to left shoulder (typically 32-38 cm).
- Sagittal (affected side): Slices should be parallel to the spinal cord in the coronal plane and parallel to the line joining the vertebral body and spinous process of the cervical spine in the axial plane.
Cover the whole affected side of the brachial plexus from the spinal cord to the shoulder.

Fig. 4: Coronal sequence planning. Slices need to be parallel to the spinal cord in the sagittal plane in order to optimally demonstrate the brachial plexus (upper row). Utilizing an incorrect angle will result to increased partial volume effects and an insufficient demonstration of the brachial plexus (middle and lower row).
References: Bac Nguyen
Sequences
a.
Gold Standard
- Conventional two-dimensional T1- and T2-weighted fast/turbo spin echo (2D T1-w and T2-w FSE/TSE) are routinely used in MRN of the brachial plexus because they are standard sequences and they are widely available. T1-w FSE acquisitions are most useful for highlighting the nerves anatomy,
thoracic outlet,
surrounding fat,
scalene and regional muscles.
T2-w FSE acquisitions are obtained with and/or without fat suppression for optimal assessment of the brachial plexus and its pathology.
STIR and Dixon/IDEAL techniques provide robust fat suppression,
whereas standard chemical fat saturation or hybrid techniques (SPIR,
SPAIR) often lead to heterogeneous fat suppression due to large FOV and magnetic field inhomogeneities (fig.
5).
- Three-dimensional fat-suppressed T1-weighted gradient echo (3D T1-w GRE) sequences are a good alternative for thin-slice imaging,
before and after the administration of a paramagnetic contrast agent (fig.
6). Routine use of intravenous contrast is not required,
unless there is a suspicion of neoplasm,
infection or diffuse polyneuropathy.
- Modified three-dimensional T2-weighted fast/turbo spin echo sequences (CUBE,
SPACE) enable the acquisition of high-resolution,
isotropic datasets (the term isotropic means that the voxel is uniform in all directions) with contrast similar to the conventional 2D FSE sequences,
in clinically acceptable acquisition times and without SAR limitations (fig.
7).
Modified 3D FSE sequences can be used with and/or without fat suppression,
however the 3D STIR acquisitions are preferred because they allow excellent background fat suppression and high-contrast multiplanar and curved planar reconstructions.
Nevertheless,
these sequences may not be available in systems with old software,
and in this case imaging should be based only on the conventional 2D FSE acquisitions.
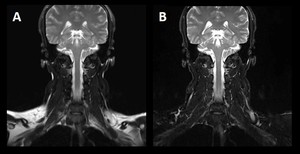
Fig. 5: Coronal T2-w FSE with chemical fat saturation (A) and coronal T2-w FSE Dixon (B) of the cervical spine and brachial plexus. Image (A) shows heterogeneous fat suppression, which reduces the image quality and may obscure pathology. Image (B) provides robust fat suppression, because the Dixon technique is insensitive to Β0 and B1 magnetic field inhomogeneities. Image dataset acquired at 1.5 Tesla.
References: Bac Nguyen
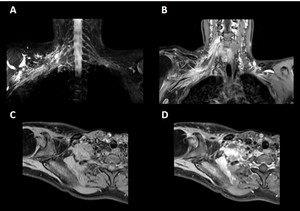
Fig. 6: Brachial plexus tumour. Coronal thin-section MIP 3D STIR (A), contrast-enhanced coronal 3D T1-w GRE water image (B), non-contrast enhanced axial 3D T1-w GRE water image (C) and contrast-enhanced axial 3D T1-w GRE water image (D). 3D T1-w GRE acquisitions offer high-resolution, thin-slice imaging before and after the administration of a paramagnetic contrast agent. Contrast uptake can be seen on (B) and (D).
References: Bac Nguyen
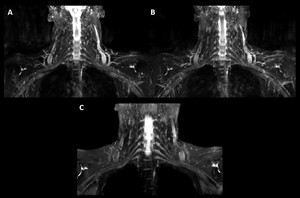
Fig. 7: Coronal thin-section MIP 2D T2-w Dixon water image (A), coronal thin-section MIP 2D STIR (B) and coronal thin-section MIP 3D STIR (C). Modified 3D STIR offers high-resolution, isotropic datasets with contrast similar to the conventional 2D acquisitions, in approximately the same scan time and without SAR limitations. Moreover note that the brachial plexus is better highlighted on (C), while the motion artifacts are more pronounced on (A) and (B).
References: Bac Nguyen
b.
Additional sequences/techniques
- Three-dimensional Double Echo Steady State sequence with water excitation technique (3D DESS WE) can provide high-quality,
high-resolution,
isotropic images of the brachial plexus (fig.
8).
3D DESS WE offers the advantage of nulled signal from the adjacent vessels,
cerebrospinal fluid (CSF) and fat,
which can greatly help in pathology detection and localization.
Unfortunately,
3D DESS WE is not available from all MR vendors,
therefore its applications are limited.
- Three-dimensional Double Inversion Recovery (3D DIR) is a volumetric acquisition that provides both fat and CSF suppression,
which leads to an improved nerve-to-background tissue contrast and enhanced ability to visualize the brachial plexus (fig.
9).
TI1 is used for the suppression of the CSF and TI2 is used for the suppression of the fat.
TI1 should be selected at 3000 msec,
while TI2 should be selected at 240 msec.
- Three-dimensional T2-weighted fast/turbo spin echo with Motion Sensitized Driven Equilibrium (MSDE) black blood pre-pulse (3D NerveVIEW) enables nerve-selective images with reduced remaining intra-lumen signal of the veins.
3D NerveVIEW offers increased depiction of smaller brachial plexus branches,
however,
this sequence is not available from all MR vendors, therefore its applications are limited.
- Contrast-enhanced modified 3D STIR can improve the CNR between the brachial plexus and its surrounding tissues,
in comparison with the standard,
non-contrast enhanced technique (fig.
10). Contrast-enhanced 3D STIR relies on the fact that the paramagnetic contrast material (based on the T2-shortening effect of gadolinium) highly decreases the signal from the veins and lymph nodes,
providing an accurate,
high-resolution,
3D display of the brachial plexus and its branches.
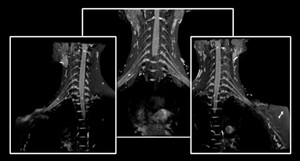
Fig. 8: Coronal thin-section MIP 3D DESS WE. 3D DESS sequence with water excitation technique provides high-resolution, isotropic imaging of the brachial plexus, with excellent visualization of the nerves. Image dataset acquired at 1.5 Tesla.
References: Bac Nguyen

Fig. 9: Inverted coronal thin-section MIP 3D STIR (A) and inverted coronal thin-section MIP 3D DIR (B). 3D DIR offers a high quality demonstration of the brachial plexus with no superimposition of the high CSF signal.
References: Bac Nguyen
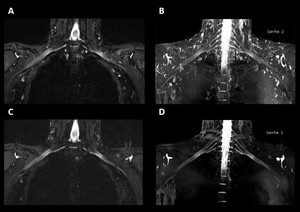
Fig. 10: Non-contrast enhanced 3D STIR (A, B) and contrast-enhanced 3D STIR (C, D) acquisitions. The contrast-enhanced technique results in improved contrast between the brachial plexus and surrounding tissues because the T2 shortening effects of the paramagnetic contrast agent suppress the signal from the vessels and lymph nodes.
References: Bac Nguyen
c.
Functional Sequences
Functional sequences,
such as DWI and DTI,
can also be helpful in MRN of the brachial plexus.
- Diffusion-Weighted Imaging (DWI) is used to evaluate the random,
thermally-induced,
microscopic water motion within a tissue,
well known as Brownian motion.
DWI offers the advantage of suppressed background structures and flowing blood in vessels,
thereby selectively highlights the nerves with high signal intensity.
In addition,
DWI is very useful to oncological cases as it provides information about tissue microarchitecture/biology (fig.
11).
The STIR technique is mainly used to provide robust fat suppression.
- Diffusion Tensor Imaging (DTI) is an extension of DWI that takes into account and measures the anisotropic diffusion (nerves are highly anisotropic).
DTI can show if a tumour deviates,
infiltrates or distructs the fiber bundles,
offering functional information.
- Nonetheless,
DWI and DTI have a relatively low spatial resolution,
can be time consuming and may suffer from image distortions,
limitations that cannot be neglected in imaging of fine structures such as peripheral nerves.

Fig. 11: Brachial plexus tumour. Coronal thin-section MIP 3D STIR (A) and coronal DWI STIR b1000 (B) with corresponding ADC map (C). The tumour presents diffusion restriction, which can assist in the characterization of the lesion. Finally, note that DWI offers the advantage of suppressed background structures (e.g. CSF, vessels).
References: Bac Nguyen
Recommended Protocol
Table 1 shows the recommended protocol for a comprehensive MR Neurography of the brachial plexus.
Note: This is a recommended protocol, based on the literature and our experience.
The specifics will vary depending on the clinical question,
MRI hardware and software,
radiologist's and referrer's preference,
institutional protocols,
patient factors (e.g.
allergy) and time constraints.
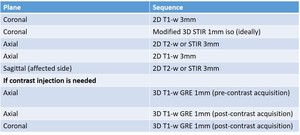
Table 1: Recommended protocol for a comprehensive, high resolution MR Neurography of the brachial plexus.
Image Post-Processing
Due to the obliquity of brachial plexus branches,
the longitudinal extent of the plexus and its related pathology is difficult to be determined on raw data images.
Multiplanar reconstruction (MPR),
curved planar reconstruction (CPR),
maximum intensity projection (MIP),
volume (VR) and cinematic (CR) rendering are used to highlight the peripheral nerves in their entirety (fig.
12).
For MPR and CPR,
isotropic (or nearly isotropic) acquisitions should be obtained.

Fig. 12: Figure shows cinematic rendering (CR) images of the brachial plexus. Cinematic rendering is a novel post-processing technique for 3D visualization of image data. Compared to the other techniques, CR results in a more photo-realistic representation of the anatomy.
References: Bac Nguyen
Artifacts,
pitfalls and solutions
Artifacts and pitfalls are common in the MRN of the brachial plexus,
resulting in degraded image quality and incorrect image interpretation.
Specifically,
MRN can suffer from:
- Increased perineural signal,
originated from the adjacent vessels,
lymph nodes and CSF. Modified 3D FSE acquisitions are mainly affected by strong background signal.
The use of additional sequences (DESS and/or DWI) and/or the utilization of intravenous contrast media can address this disadvantage (fig.
10).
- Inhomogeneous fat suppression,
when chemical fat saturation or hybrid techniques are used.
STIR and Dixon techniques can resolve this issue,
offering robust fat suppression (fig.
5).
- Susceptibility artifacts,
especially at 3T.
FSE acquisitions with the lowest possible TE and echo spacing (ESP),
and high receiver bandwidth (rBW) can reduce this type of artifacts.
Patients with metallic implants should be scanned at 1.5T.
- Motion artifacts.
Preparation,
positioning and communication with the patient,
are crucial for obtaining high quality,
high resolution images of the brachial plexus.
Moreover,
the implementation of modified 3D STIR instead of the conventional 2D STIR or T2-w Dixon/IDEAL can reduce the motion and flow artifacts (fig.
7).
- Chemical shift artifacts,
especially at 3T.
FSE acquisitions,
in-phase TEs,
high rBW and fat suppression should be selected in order to overcome chemical shift artifacts.
- Magic angle effect.
This effect can be eliminated with higher TE values or re-positioning of the patient.
Clinical utility
MRN of the brachial plexus is indicated in the following situations:
- Brachial plexopathy
- Brachial plexus tumour (primary or secondary)
- Image-guided treatment planning (surgical or radiation)
- Brachial plexus injury
- Diffuse polyneuropathy
-
Non-specific shoulder and arm pain or weakness,
in which EMG and traditional cervical spine MRI are inconclusive
-
Anatomy and nerve abnormalities evaluation in patients under consideration for thoracic outlet syndrome (TOS) surgery
- Evaluation of nerve re-entrapment/persistent impingement in failed surgery cases
- Planning for MRI–guided administration of pain medication

. Utilizing an incorrect angle will result to increased partial volume effects and an insufficient demonstration of the brachial plexus (middle and lower row). References: Bac Nguyen")
 and coronal T2-w FSE Dixon (B) of the cervical spine and brachial plexus. Image (A) shows heterogeneous fat suppression, which reduces the image quality and may obscure pathology. Image (B) provides robust fat suppression, because the Dixon technique is insensitive to Β0 and B1 magnetic field inhomogeneities. Image dataset acquired at 1.5 Tesla. References: Bac Nguyen")
, contrast-enhanced coronal 3D T1-w GRE water image (B), non-contrast enhanced axial 3D T1-w GRE water image (C) and contrast-enhanced axial 3D T1-w GRE water image (D). 3D T1-w GRE acquisitions offer high-resolution, thin-slice imaging before and after the administration of a paramagnetic contrast agent. Contrast uptake can be seen on (B) and (D). References: Bac Nguyen")
, coronal thin-section MIP 2D STIR (B) and coronal thin-section MIP 3D STIR (C). Modified 3D STIR offers high-resolution, isotropic datasets with contrast similar to the conventional 2D acquisitions, in approximately the same scan time and without SAR limitations. Moreover note that the brachial plexus is better highlighted on (C), while the motion artifacts are more pronounced on (A) and (B). References: Bac Nguyen")

 and inverted coronal thin-section MIP 3D DIR (B). 3D DIR offers a high quality demonstration of the brachial plexus with no superimposition of the high CSF signal.
References: Bac Nguyen")
 and contrast-enhanced 3D STIR (C, D) acquisitions. The contrast-enhanced technique results in improved contrast between the brachial plexus and surrounding tissues because the T2 shortening effects of the paramagnetic contrast agent suppress the signal from the vessels and lymph nodes. References: Bac Nguyen")
 and coronal DWI STIR b1000 (B) with corresponding ADC map (C). The tumour presents diffusion restriction, which can assist in the characterization of the lesion. Finally, note that DWI offers the advantage of suppressed background structures (e.g. CSF, vessels). References: Bac Nguyen")
 images of the brachial plexus. Cinematic rendering is a novel post-processing technique for 3D visualization of image data. Compared to the other techniques, CR results in a more photo-realistic representation of the anatomy. References: Bac Nguyen")
