ECR 2019 / C-2475
All above female pelvis: benign gynecological pathology in MRI
Congress:
ECR 2019
Poster Number:
C-2475
Type:
Educational Exhibit
Keywords:
Education, MR, Genital / Reproductive system female, Pathology
Authors:
I. Diez, L. GARCIA DEL SALTO, A. Marco Sanz, F. Aguilera del Hoyo, J. de Miguel Criado, P. Fraga, P. Quintana Valcarcel; MADRID/ES
DOI:
10.26044/ecr2019/C-2475

Fig. 2:
Coronal T2 Anatomical Uterus

Fig. 3:
Axial T2 Anatomical Uterus: retroversion left
.
 and B): secretory phase with increased thickness of the junction line and C):proliferative phase with better delimited Union line")
Fig. 4:
Sagittal T2 Uterus: A) and B): secretory phase with increased thickness of the...
 sagittal T2 (Red Arrows). B) Axial T1 saturation fat (yellow arrows).")
Fig. 5:
Normal cervix. A) sagittal T2 (Red Arrows). B) Axial T1 saturation fat (yellow...
 and coronal T2 (B): Complete uterine agenesis and the upper two-thirds of the vagina (red arrows) with pelvic ectopic kidney (yellow arrows).")
Fig. 7:
Mayer-Rokitansky-Küster-Hauser syndrome. Sagittal (A) and coronal T2 (B):...
 and B) and Axial T2 C) and D). Didelfal uterus with two uterus and two divergent necks.")
Fig. 8:
Coronal T2 A) and B) and Axial T2 C) and D). Didelfal uterus with two uterus...

Fig. 9:
Axial T2. Bicorn complete bicollis uterus with septum reaching to the outer...
 and fibrotic linear image until cervix (red arrow). Axial T2 and B) and C) coronal T2.")
Fig. 10:
Septate uterus: Presence of muscular septum at the height of the fundus (blue...

Fig. 11:
Coronal T2. Arcuate uterus. Cleft in the endometrial cavity at the height of...
 in patients with intramural uterine myoma (yellow arrow) and left hydrosalpinx (blue arrow).")
Fig. 12:
Coronal T2. Endometrial polyp (red arrow) in patients with intramural uterine...
 and B) T2 sagital and C) coronal sequences. Intramural (yellow arrow), submucosal (red arrow), subseroso (blue arrow)and pediculated myoma (white arrow). Markedly hypointense in T2 and some área of high signal by hyaline degeneration")
Fig. 13:
Location of myioma, A) and B) T2 sagital and C) coronal sequences. Intramural...
 in patient with surgical antecedents of previous right anexectomía. Vascular pedicle dependent on the cervical isthmus (yellow arrow)")
Fig. 14:
Axial T2. Parasitic myoma (blue arrow) in patient with surgical antecedents of...
 and intramural (yellow arrow). Cervical nabothian cysts (blue arrow).")
Fig. 15:
Sagittal T2. Hypointense, subserous myoma (red arrow) and intramural (yellow...
 and subserous (white arrow), axial sequences T2 (A) and axial T1 saturation fat with intravenous contrast (B): homogeneous contrast capture.")
Fig. 16:
Intramural myomas (red Arrow) and subserous (white arrow), axial sequences T2...
 in coronal T2 (A) and sagittal sequence T2 (B) in patient with ovarian neoformativo process (red arrow head) and hyperintense foci in coronal T1 with and without contrast intravenous (C and D) by menstrual bleeding, in relation to diffuse adenomyosis")
Fig. 17:
Thickening of the binding line with myometrium and hyperintense foci in T2...
; C and D) coronal T2 and E) axial T1 saturation fat.")
Fig. 18:
Thickening of the binding line with myometrium and hyperintense foci in T2, in...
, Axial T2 (B and E), axial T1 saturation fat (D) and axial T1 (F). Focal adenomyosis (red rrows) in patients with right ovarian teratoma (blue arrows) and left follicular cyst (yellow arrows).")
Fig. 19:
Hyperintense foci in T2 that correspond to dilated endometrial glands, in...
 Sagittal and B) coronal T2 and C) sagital T2.")
Fig. 20:
Nabothian cysts in two different patients. A) Sagittal and B) coronal T2 and C)...
 and markedly hypointense solid mass in cervical T2 that protrudes in vagina, intramural, in relation to cervical leiomyoma (yellow arrows). Coronal T2 (A) and sagittal T2 (B and C)")
Fig. 21:
Uterine myoma intramural left ridge (red arrow) and markedly hypointense solid...
 coronal and B) sagittal plane.")
Fig. 22:
Isthmic cervical myoma of lobulated morphology that protrudes inserted into...
 and right attached (blue arrow). A) and B) sagittal T2 and C) axial T2.")
Fig. 23:
Functional cyst in the right annex (yellow arrow) and right attached (blue...
 and left Adnexal follicular cyst (yellow arrow). Axial T2 A) and axial T1 B) and T1 saturation fat C).")
Fig. 24:
Right Paraovarian cyst (red arrow) and left Adnexal follicular cyst (yellow...
. Right hydrosalpinx (yellow arrow) in patient studying for cervical cancer (red arrow).")
Fig. 25:
Axial T2. (A and B). Right hydrosalpinx (yellow arrow) in patient studying for...
 and right piosalpinx (yellow arrow). Left follicular cyst (red arrow). A) Axial T2 and B) axial T1 saturation fat with intravenous contrast.")
Fig. 26:
Pelvic inflammatory disease: ovarian abscess (blue arrow) and right piosalpinx...
 in patient with hyperandrogenism")
Fig. 27:
SOP coronal T2 image. Multiple small peripheral cysts on right annex (yellow...
 and left Hydrosalpinx (yellow arrow) in sequence T1 saturation coronal fat (A) and axial (B) and T2 coronal (C) and axial (D), where endometrial polyp is also displayed.")
Fig. 28:
Endometrioma (red arrow) and left Hydrosalpinx (yellow arrow) in sequence T1...
, ovarian endometriomata with blood in different stages (red Arrows) and peritoneum (blue arrows). A) sagittal T2 with hypointense thickening of the uterus-sacral ligament. B and C) coronal T2 with bilateral ovarian endometriomata with metahemoglobin shading effect. D and E) axial T1 saturation fat which reveals acute bleeding in annexes, straight-vaginal septum and blood peritoneum")
Fig. 29:
Ovarian endometriosis, of the rectus-vaginal septum, and thickening of the...
, thickening of the uterus-sacral ligaments in its proximal portion (red arrow) and Endometriotic foci in Douglas (yellow arrow) located at the bottom of the Douglas Sac. A and B Axial T2 and T1. C) sagittal t1 saturation fat and D) axial T1 saturation fat.")
Fig. 30:
Subperitoneal localization implants in patients with deep endometriosis....
 coronal plane T1 saturation fat with intravenous contrast. B) coronal plane and C) sagittal plane in T2 sequence.")
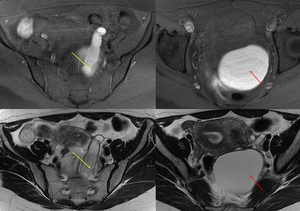
Fig. 31:
Cystadenoma mucinous right ovary. Multilocular cystic lesion with fine septa...

Fig. 32:
Benign gynecological Pathology

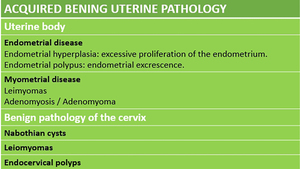
Fig. 33:
Acquired bening uterine pathology

Fig. 34:
Bening ovarian injures

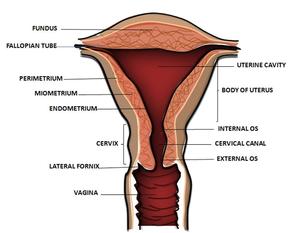
Fig. 1:
Uterine anatomy

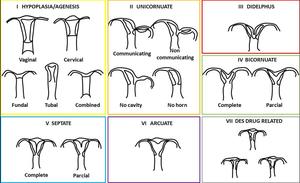
Fig. 6:
Classification of the malformations of the Müller and Gibbons ducts modified