ECR 2019 / C-2486
Pancreatic Pseudotumors: Lesions that can mimic primary pancreatic neoplasms.
Congress:
ECR 2019
Poster Number:
C-2486
Type:
Educational Exhibit
Keywords:
Education and training, Education, MR, CT, Pancreas, Gastrointestinal tract, Abdomen
Authors:
D. Strabelli, L. Coura, G. A. B. G. Bandeira, M. H. Verussa, I. S. Oliveira, M. D. S. Rocha; São Paulo/BR
DOI:
10.26044/ecr2019/C-2486
 and biliary system arise from the hepatic diverticulum. The dorsal pancreatic bud (arrowhead in 3A and 3B) arises from the dorsal mesogastrium. After clockwise rotation of the ventral bud around the caudal part of the foregut, there is fusion of the dorsal pancreas (located anterior) and ventral pancreas (located posterior), shown in image 3C.
Image 3D illustrate fusion of the ventral and dorsal pancreatic ducts. Pancreas drain predominantly through the ventral duct, which joins the common bile duct at the level of the major papilla. The dorsal duct empties at the level of the minor papilla.")
Fig. 3:
Drawings illustrate the embryologic development of the pancreas and biliary...
. 4C and D: At coronal images this area configurates a tubular structure and corresponds to the duodenum, completely surrounded by pancreatic tissue (yellow arrow), making the diagnosis of an annular pancreas. Annular pancreas is a rare congenital anomaly, in which a portion of the pancreas involves partially or completely the duodenum, secondary to incomplete rotation of the ventral pancreatic bud.")
Fig. 4:
4A and B: Axial CT images on arterial phase show a hypovascular area in the...
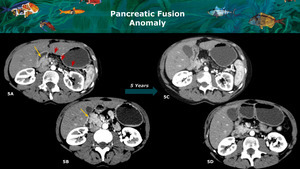
, and diffuse fat replacement of the body and tail (red arrows) with an abrupt change, findings that should raise suspicion for a pancreatic neoplasia. Note there is no main pancreatic duct dilatation. In a follow-up scan 5 years later, no significant changes were seen (CT axial views on arterial phase images - 5C and 5D). Those findings suggest a pancreatic fusion anomaly with fat replacement of the dorsal pancreas and preservation of the ventral parenchyma.")
Fig. 5:
5A and 5B: CT axial images on arterial phase show normal appearance of the...
 that confirmed the presence of splenic tissue (pointed by red arrows). An intrapancreatic accessory spleen typically is a small well-defined mass, usually found in the pancreatic tail, which can mimic an hypervascular neoplastic pancreatic lesion. It follows the density, signal intensity, and enhancement pattern of the spleen on all CT phases and MRI sequences.")
Fig. 6:
6A and B: Axial views on arterial phase CT show a hypervascular well defined...
. Coronal T2 image (7C) better evidences the relationship with the pancreatic tail (yellow arrow). 7E and F: Note the hypervascular aspect of the lesion in the T1 post contrast arterial MRI sequences.
7D: The patient was also submitted to further nuclear imaging scan, that confirmed the uptake of technetium 99–labelled red blood cells and the presence of splenic tissue.")
Fig. 7:
Another case of an accessory spleen, this time simulating an pancreatic tail...
, with no main pancreatic duct dilation or distal parenchymal atrophy. T1 weighted in- and out-phase axial images (8C and 8D) show a signal drop in this area (yellow arrow), implying intracytoplasmic lipid content. The images illustrate a case of uneven pancreatic fat deposition, sometimes related to the fact that the ventral and dorsal portions of the gland demonstrate different histologic compositions. Focal sparing of the peribiliary region with fatty replacement of the anterior portion of the pancreatic head is a common finding on imaging studies.")
Fig. 8:
CT arterial and portal venous phases axial views evidence an hypoattenuating...
. C, D and E: T1-weighted pre contrast (C) and dynamic sequences (D,E) reveal a normal signal in the head of the pancreas (yellow arrows) and progressive enhancement of the retroperitoneal lesion (red arrows). This patient was submitted to surgical resection and the lesion was proved to be a desmoid tumor compressing the pancreatic parenchyma.")
Fig. 9:
A and B: MRI T2W and diffusion images show a solid well circumscribed...
 simulating an adenocarcinoma. C, D and E: CT axial, sagittal and coronal reconstructions show that the lesion was arising from gastric small curvature wall (red arrows) and compressing pancreatic parenchyma (yellow arrow), that remains with normal enhancement and size. This demonstrates the importance of using reconstructions in CT to analyze pancreas relations and identify the real origin of the lesions.")
Fig. 10:
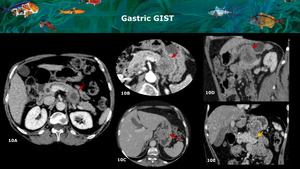
A and B: CT axial show a partially necrotic solid mass within the pancreatic...
, a finding that might be confused with a cystic pancreatic lesion, especially if small and fluid-filled. B: MRI axial T2-weighted fat suppressed image. Note that this lesion has a fluid level (yellow arrow), the hint to consider that is originating from a bowel loop.")
Fig. 11:
A: MRI axial T2-weighted image shows a duodenal diverticulum arising from the...
. B: CT sagittal reconstruction evidences that the mass was in fact extrapancreatic and superiorly compresses the pancreas parenchyma (yellow arrow). C: CT axial in a superior level demonstrate that the lesion was originated from the caudate liver lobe (red arrow). D: CT axial on an inferior level show normal parenchyma throughout all the pancreas. This patient had chronic liver disease with a final diagnosis of infiltrative hepatocellular carcinoma (a lesion arising from caudate lobe and compressing pancreas head).")
Fig. 12:
A: CT axial show hypovascular solid mass in the pancreas head (red arrow). B:...
. C and D: On the same CT and FDG-PET scans, a circumferential thickening of the gastric antrum wall is depicted (red arrows), also with high FDG uptake. This was proven to be a gastric lymphoma on pathology with a peripancreatic lymph node, adjacent the pancreatic head.")
Fig. 13:
A and B: CT post contrast and FDG-PET CT images show a ill-defined hypovascular...
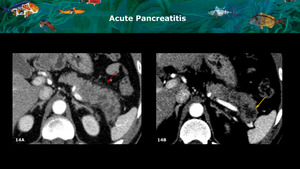
, and enlargement of the pancreatic tail, with intrapancreatic hypovascular or necrotic areas (yellow arrow). This patient had a history of abdominal pain for over 4 weeks and elevated serum amylase and lipase, confirming the hypothesis of an acute pancreatitis. It is important to highlight that without those informations the differential diagnosis with a cystic neoplasm is not possible.")
Fig. 14:
A and B: CT arterial phase axial images show peripancreatic fat stranding (red...
 associated to peripancreatic and retroperitoneal fat stranding and fluid (yellow arrows) in a patient with blunt force trauma.")
Fig. 15:
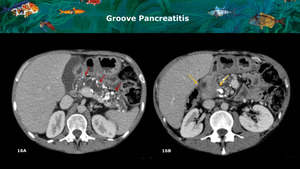
A and B: CT axial arterial and portal phases images show a hypoperfused linear...
. B: An hypovascular solid mass is identified occupying the paraduodenal sulc (yellow arrows), raising the suspicion of pancreas adenocarcinoma. This patient was submitted to surgical resection due to abdominal pain and no neoplastic cells were found.")
Fig. 16:
A: CT axial portal phase images show chronic pancreatitis characterized by main...
, along with diffuse pancreas enlargement, loss of the normal lobulated contours and peripancreatic rim of low attenuation (yellow arrow), classic findings of autoimmune pancreatitis.")
Fig. 17:
A and B: CT axial arterial phase images show hypocontrastant areas within the...
.
B: Axial, coronal and sagittal reconstructions show a solid and partially necrotic mass in the pancreas head (yellow dotted arrows), occupying the superior mesenteric vein location and in proximity to the superior mesenteric artery (blue dotted artery), indicating that the mass was originating from the vein.
C: Axial venous phase. Note that superior mesenteric vein is not characterized and there are jejunal ingurgitated veins (blue arrows) in left hipocondrie. This patient had a complicated appendicitis with SMV thrombophlebitis.
D: Coronal reconstruction shows lymph nodes and the inflammatory tissue in SMV path (yellow arrows). Superior mesenteric artery (blue dotted arrow).
Follow-up CT performed one (E) and nine (F) months after the initial CT. After appendicectomy and clinical treatment, there was completely remission of the inflammatory mass (red dashed arrows).")
Fig. 18:
A: CT axial arterial phase images show normal appearance of the pancreas body...
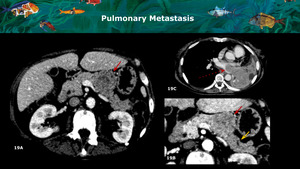
 proven to be a solitary pulmonary metastasis. Note the abrupt change in the parenchymal attenuation distal to the lesion (yellow arrow) and the normal parenchyma in the head, findings that can also be found in pancreatic adenocarcinoma.
C: Pulmonary infiltrative mass corresponding to the primary tumor (red dotted arrow).")
Fig. 19:
A and B: Axial CT images on portal venous and arterial phase demonstrate a...
 seen in arterial phase axial CT images (yellow arrow).
B: Arterial phase axial CT images show an hypovascular mass in the tail of the pancreas (red arrow), proven to be metastatic lesion from the renal cell carcinoma. Multiple necrotic metastatic lesions are also present in the liver (yellow dotted arrow).
C: In the magnified arterial phase axial images, atrophy of the parenchyma in the tail is better depicted (red dotted arrow).")
Fig. 20:
A: Left kidney hypervascular mass corresponding to a renal cell carcinoma...
 on axial CECT images, proven to be metastatic lesions from ovarian mucinous adenocarcinoma.
B and C: Coronal and axial CECT images demonstrate a large cystic lesion arising from the pelvis along the right gonadal vessels (yellow arrow), corresponding to the primary tumor.")
Fig. 21:
A: Hypoattenuating lesions within the pancreas tail and adjacent to the...