ECR 2019 / C-2611
Peritoneal metastases – role of diagnostic imaging in therapeutic decision-making process
Congress:
ECR 2019
Poster Number:
C-2611
Type:
Educational Exhibit
Keywords:
Cancer, Structured reporting, Staging, Diagnostic procedure, MR-Diffusion/Perfusion, MR, CT, Peritoneum, Oncology, Abdomen, Metastases
Authors:
M. A. Szadkowska1, J. Pałucki1, J. Podgorska2, A. Cieszanowski1; 1Warsaw/PL, 2Warszawa/PL
DOI:
10.26044/ecr2019/C-2611
 and ADC map (right).")
Fig. 1:
Ovarian cancer. Peritoneal metastases in the pouch of Douglas. DW-MRI, b=800...

Fig. 2:
Serous ovarian cancer after three cycles of chemotherapy. Peritoneal metastases...

Fig. 3:
Massive ascites and peritoneal metastases in the right paracolic gutter in a...

Fig. 4:
61-year-old patient with uterine adenocarcinoma G3. Increased density of the...

Fig. 5:
62-year-old patient with clear cell ovarian cancer. Confluent nodules in the...

Fig. 6:
Omental cake.

Fig. 7:
62-year-old patient with clear cell ovarian cancer. Nodular thickening of...

Fig. 8:
Pseudomyxoma peritonei. Scalloping of the liver and the spleen surface.

Fig. 9:
Serous ovarian cancer. Liver subcapsular implants.

Fig. 10:
47-year-old patient with ovarian adenocarcinoma. Implants in the left paracolic...

Fig. 11:
Malignant melanoma. Peritoneal metastasis in the greater omentum.

Fig. 12:
47-year-old patient with ovarian adenocarcinoma. Sigmoidostomy. Peritoneal...

Fig. 13:
47-year-old patient with ovarian adenocarcinoma. Another involved segment of...

Fig. 14:
Enlarged cardiophrenic lymph nodes.

Fig. 15:
47-year-old patient with ovarian adenocarcinoma. Subcapsular splenic lesions.

Fig. 16:
47-year-old patient with ovarian adenocarcinoma. Peritoneal lesions involving...

Fig. 17:
Serous ovarian cancer. Pleural fluid, partially walled-off on the left side –...

Fig. 18:
PCI-score – created basing on Jacquet P, Sugarbaker PH. Clinical research...

Table 1:
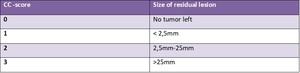
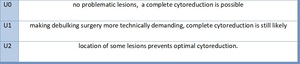
CC - score - created basing on Jacquet P, Sugarbaker PH. "Clinical research...
 and intra-operative hyperthermia for digestive cancers with peritoneal carcinomatosis."")
Table 6:
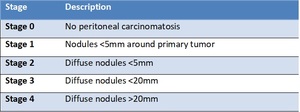
Gilly's peritoneal carcinomatosis staging - created basing on Gilly FN, Carry...

Table 5:
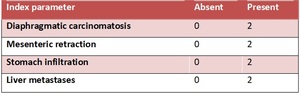
Modified Fagotti score - created basing on Brun JL, Rouzier R, Uzan S, Daraï...

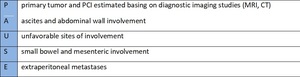
Table 7:
PAUSE - adapted from Chandramohan A1, Thrower A2, Smith SA2, Shah N2, Moran...

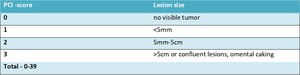
Table 2:
PCI score - created basing on Jacquet P, Sugarbaker PH. Clinical research...

Table 8:
PAUSE - adapted from Chandramohan A1, Thrower A2, Smith SA2, Shah N2, Moran...

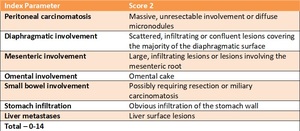
Table 4:
Fagotti score - created basing on Fagotti A, Ferrandina G, Fanfani F, et al....

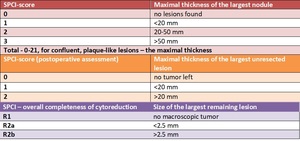
Table 3:
SPCI-score- created basing on Verwaal VJ, van Tinteren H, van Ruth S, et al....