ECR 2019 / C-2640
Keep calm and take a deep breath: a pictorial essay of the main findings in lung congenital malformations
Congress:
ECR 2019
Poster Number:
C-2640
Type:
Educational Exhibit
Keywords:
Congenital, Intrauterine diagnosis, Ultrasound-Colour Doppler, MR, Thorax, Foetal imaging
Authors:
E. Di Puglia1, T. Fazecas1, R. Nogueira1, H. WERNER JÚNIOR1, P. A. N. Daltro1, B. GUEDES RIBEIRO1, M. G. M. Waksman2, E. Antunes1, C. L. Leidersnaider1; 1Rio de Janeiro/BR, 2Petrópolis, RJ/BR
DOI:
10.26044/ecr2019/C-2640

Fig. 3:
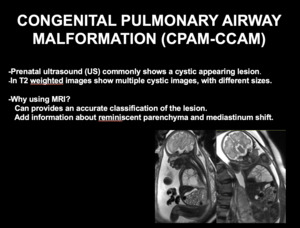
INTRODUCTION CONGENITAL PULMONARY AIRWAY MALFORMATION

Fig. 4:
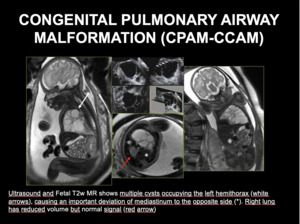
US AND MRI IN CONGENITAL PULMONARY AIRWAY MALFORMATION.
. Ultrasound and Fetal T2w MR shows multiple cysts occupying the left hemithorax (white arrows), causing an important deviation of mediastinum to the opposite side (*). Right lung has reduced volume but normal signal (red arrow)")
Fig. 5:
CONGENITAL PULMONARY AIRWAY MALFORMATION (CPAM-CCAM). Ultrasound and Fetal T2w...
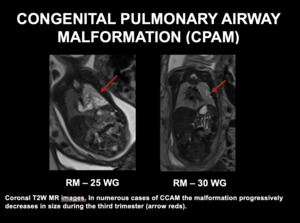
. Coronal T2W MR images. In numerous cases of CCAM the malformation progressively decreases in size during the third trimester (arrow reds).")
Fig. 6:
CONGENITAL PULMONARY AIRWAY MALFORMATION (CPAM-CCAM). Coronal T2W MR images. In...

Fig. 7:
BRONCHOGENIC CYST

Fig. 8:
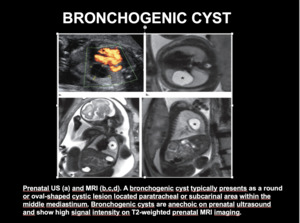
BRONCHOGENIC CYST. A bronchogenic cyst typically presents as a round or...

Fig. 9:
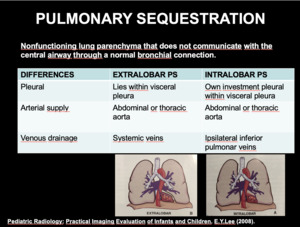
EXTRALOBAR AND INTRALOBAR PULMONARY SEQUESTRATION

Fig. 10:
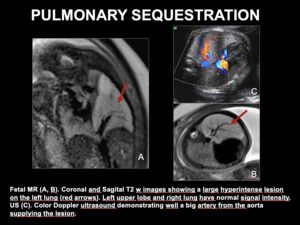
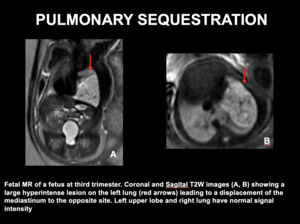
PULMONARY SEQUESTRATION
. Coronal and Sagital T2 w images showing a large hyperintense lesion on the left lung (red arrows). Left upper lobe and right lung have normal signal intensity.
US (C). Color Doppler ultrasound demonstrating well a big artery from the aorta supplying the lesion.")
Fig. 11:
PULMONARY SEQUESTRATION. Fetal MR (A, B). Coronal and Sagital T2 w images...
 leading to a displacement of the mediastinum to the opposite site. Left upper lobe and right lung have normal signal intensity")
Fig. 12:
PULMONARY SEQUESTRATION - Fetal MR of a fetus at third trimester. Coronal and...

Fig. 13:
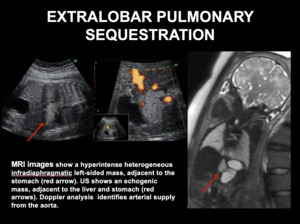
EXTRALOBAR PULMONARY SEQUESTRATION

Fig. 14:
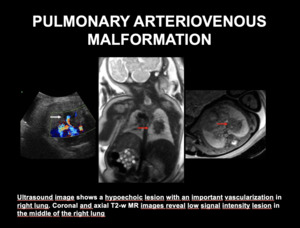
PULMONARY ARTERIOVENOUS MALFORMATION

Fig. 15:
PULMONARY ARTERIOVENOUS MALFORMATION - Ultrasound image shows a hypoechoic...