ECR 2019 / C-2641
Colitis: infectious, ischemic or inflammatory? The good, the bad and the ugly
Congress:
ECR 2019
Poster Number:
C-2641
Type:
Educational Exhibit
Keywords:
Colon, Abdomen, CT, MR-Enterography, Ultrasound, Contrast agent-intravenous, Diagnostic procedure, Inflammation, Ischaemia / Infarction, Infection
Authors:
C. Idoate Ortueta, A. Verón Sánchez, I. GALÁN GONZALEZ, J. M. MUÑOZ OLMEDO, C. DE BENAVIDES BERNALDO DE QUIRÓS; Madrid/ES
DOI:
10.26044/ecr2019/C-2641

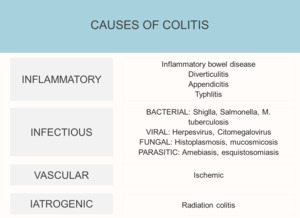
Fig. 1:
Causes of colitis

Fig. 2:
Enhancement patterns. White and gray attenuation pattern.

Fig. 3:
Enhancement patterns. Water halo and fat halo signs.

Fig. 4:
Enhancement patterns. Black attenuation or pneumatosis.

Fig. 5:
Intraluminal blood indicates hemorrhage