♦ Technique of uterine AVM embolization: (6,
8,14)
- Procedure is done under local anesthesia maintaining strict aseptic precautions.
- Unilateral/bilateral femoral artery access is taken followed by 4 or 5-French introducer sheath placement at each puncture site.
- Bilateral punctures allow simultaneous angiography of both uterine arteries with subsequent overall radiation dose reduction.
- A 5 F Uterine Artery Catheter and 0.032” Terumo glide wire combination is used to perform internal iliac artery angiogram on either side.
- Alternatively,
4 F catheters like Simmons,
renal double curve or cobra may be used.
- After internal iliac artery angiogram,
selective cannulation of the uterine arteries is done.
Super selective cannulation of the uterine artery may also be done using coaxial microcatheter.
- Advance the catheter well into the uterine artery beyond any identifiable branches in the transverse segment to avoid non-target embolization.
Vessel spasm may follow,
hence balance between ideal catheter position and avoidance of spasm is needed.
- Spasm results in false end point with recanalization after catheter removal.
- Preembolization selective angiography is done to see AVM nidus size,
arteriovenous transit time,
and any functioning arterial branches distal to the microcatheter.
- Embolization can be done using Polyvinyl alcohol(PVA) particles,
glue,
gelfoam,
coils or their combinations.
- The choice of embolic material depends on the anatomic appearance of the vessels,
rate of flow and operator expertise.
- The embolic material is injected in small aliquots until stasis or reduction of flow in the AVM is achieved.
♦ Angiographic findings: (6,
9)
- Hypertrophied uterine arteries feeding tortuous hypertrophied arterial mass,
accessory feeding vessels and early draining veins.
- Aquired AVM: Single direct communication to the venous structure.
- Congenital AVM: Contrast filling of vascular plexus or a nidus and feeders from extrauterine pelvic arterial branches.
♦ Embolizing agents: (6)
- Size: 300-500/500-710 microns most commonly used.
- Used when selective cannulation of the nidus and feeding vessels is technically not possible.
- Particles less than 500-micron size are more likely to cross utero-ovarian anastomosis and can lead to ovarian failure.
- Combination of glue with lipiodol used in ratio of 1:2-1:3.
- Mixture is injected in small aliquots into the nidus of the AVM along with 5% dextrose using a sandwich technique.
(Dextrose-glue-dextrose).
- A glue cast is formed in the network arteries once the mixture is injected.
- Not preferred.
- Lead to more proximal occlusion in the vascular bed permitting collateral flow and thus recurrence.
- Also,there is loss of subsequent access to the main vessel in case of recurrence.
- Used when selective cannulation of the feeding arteries is not possible.
♦ Outcomes: (10,
15)
- Uterine AVM is a rare entity with very few case reports,
series and review articles.
- The clinical success rate of TAE in the published case reports is greater than 90%.
- Issue of ovarian dysfunction and successful pregnancy following arterial embolization is still controversial.
- Transient ovarian dysfunction has been reported in a few cases with patients having normal menstrual cycle weeks to months later.
- Thus,
handful of documented case reports do describe full term pregnancy after TAE and currently there is no strong evidence to suggest persistent ovarian failure,
pregnancy complications or fetal growth restriction post TAE.
- In an extensive systemic review carried out by Peitsidis et al on studies dating from 1954 to 2011(total of 100 cases) with acquired uterine AVM,
a recurrence rate of 17 % was reported following initial uterine artery embolization.
♦ Complications: (6,8,
10)
1.
Non-target embolization:
• Pulmonary embolism of the glue [Fig. 8]
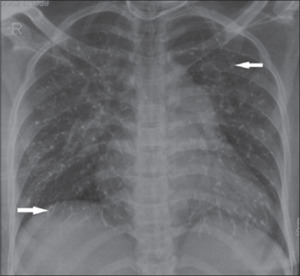
Fig. 8: Chest Radiograph of a woman with uterine AVM. Patient developed shortness of breath immediately post glue embolisation. Chest X-ray shows prominant pulmonary bay with bilaterally scattered multiple branching reticular radio densities (arrow) suggesting glue embolization.
References: Agarwal, Neha, et al. "Congenital Uterine Arteriovenous Malformation Presenting as Postcoital bleeding: A Rare Presentation of a Rare Clinical Condition." Journal of clinical imaging science 7 (2017).
• Skin necrosis
• Occlusion of vascular supply to adjacent organs
2.
Myometrial injury: rare,
suspected if persistent pain 4-5 days post embolization.
3.Uterine necrosis,
abscess formation
4.Ovarian failure: due to inadvertent flow of embolic material in the ovarian artery.
5.
Post embolization syndrome: Fever,
pain,
leukocytosis
6.
Puncture site hematoma,
puncture site AV fistula
Causes of recurrence: (16)
- Incomplete embolization
- Recanalization of the embolized vessel
- Development of collateral channels
- Uterine artery spasm during procedure interpreted as false end point
- Gestational trophoblastic disease/ choriocarcinoma as the underlying cause of uterine AVM
We present 3 cases of uterine AVM managed by endovascular approach using embolization.
All 3 patients had history of previous pregnancies/uterine instrumentation.
Endovascular approach used as an alternative to surgery since:
- Patients were unwilling for hysterectomy
- Two of the patients desired to preserve fertility in view of future pregnancy.
# CASE 1:
29 years old,
P2L2
|
History
|
|
Management
|
|
1st pregnancy
|
Uneventful
|
C -section
|
|
2nd pregnancy
|
Uneventful
|
C-section & tubectomy
|
|
Menorrhagia+urinary incontinence
|
|
Further evaluation with imaging
|
- Transabdominal USG and doppler:
- Bulky uterus with increased vascularity and high flow vessels.
- Focal myometrial mass with heterogeneous signal intensity in the antero-inferior portion of the uterus with serpiginous flow voids.[Fig. 9 ]. A diagnosis of uterine AVM was made.
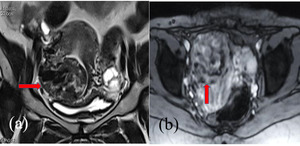
Fig. 9: MRI T2 weighted coronal image(a) showing heterogeneous signal intensity focal mass in the antero-inferior uterine wall with blooming on T2* image(b)
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
- Large uterine AVM with supply from bilateral hypertrophied uterine arteries.
- A nidus with multiple small feeding vessels and early venous drainage in internal iliac veins.
The uterine arteries were selectively cathterised and AVM was embolised with glue followed by PVA particles.[ Fig. 10, Fig. 11,
Fig. 12]
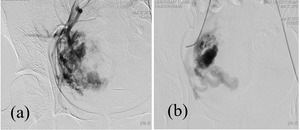
Fig. 10: Right internal iliac artery DSA showing large uterine AVM with supply from the right uterine artery, multiple small feeder vessels (a) and filling of early draining veins.(b)
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733

Fig. 11: Selective right uterine artery check angiogram post embolisation showing reduction of flow in the AVM with glue cast within the vessel bed.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
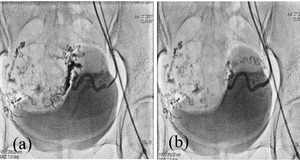
Fig. 12: Selective Left uterine artery angiogram demonstrates feeder vessels to the uterine AVM(a) and post embolisation image showing reduction in supply to the AVM with glue cast in the vessel bed.(b)
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
One and half month later:
- Recurrence of symptoms.
- Repeat Angiogram:No significant flow in the AVM through right uterine branches.
- Left uterine artery angiogram: residual AVM supplied by feeders from left uterine artery with drainage into a large venous channel. [Fig. 13]

Fig. 13: (a) Repeat DSA through Right internal iliac artery one and half month later shows no flow to the AVM from the right uterine artery. Note the glue cast from previous embolization within the vessel bed.(b) Selective left uterine artery angiogram demonstrates residual AVM supplied through hypertrophied tortuous left uterine artery branches and early drainage into right internal iliac vein.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
- Repeat embolization done with glue.
[Fig. 14]

Fig. 14: Post embolization check angiogram demonstrating marked reduction of flow in the AVM with glue cast in the network arteries.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
# Case 2:
33 year old,
P1L1A1
|
History
|
|
Management
|
|
1st pregnancy
|
Uneventful
|
C-section
|
|
2nd pregnancy
|
D&C with heavy bleeding |
Medical Management
|
|
3rd pregnancy
|
Foetus in lower uterine segment
|
D&C with resultant heavy bleeding.
Further evaluation with imaging.
|
- Transvaginal USG and colour doppler:
- Bulky uterus and increased vascularity predominantly in the posterolateral wall.
- Uterine AVM with prominent flow voids in the posterolateral wall of the uterine body indentating and displacing the endometrium.
- Nidus formed by entangled serpiginous abnormal vessel with supply from bilateral uterine arteries and early venous drainage. [Fig. 15]
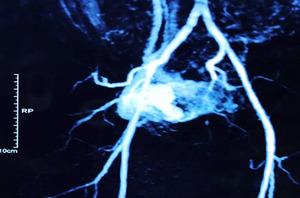
Fig. 15: MRA shows the AVM nidus formed by entangled serpiginous abnormal vessel with supply from bilateral uterine arteries and early venous drainage.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
- Hypertrophied uterine arteries supplying a large AVM with cluster of entangled feeding vessels and early venous drainage into the internal iliac veins.
Embolization done with glue and PVA particles.
[Fig. 16 ,
Fig. 17]
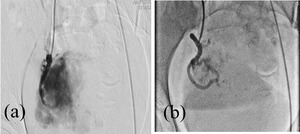
Fig. 16: Selective right uterine artery angiogram (a) demonstrates a large AVM with nidus. (b) Post embolization check angiogram showing significant reduction of flow in the AVM.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
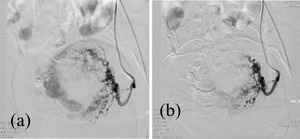
Fig. 17: (a) Selective Left uterine artery angiogram showing hypertrophied left uterine artery supplying feeder artery branches to the AVM (b) Post embolization check angiogram shows stasis and reduction of flow in the AVM. Also noted is the glue cast in the vessel bed.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
# CASE 3:
24 year old,
G4A2E1
|
History
|
|
Management
|
|
1st pregnancy
|
spontaneous abortion
|
Medical management
|
|
2nd pregnancy
|
Ectopic
|
Laparotomy
|
|
3rd pregnancy
|
Missed abortion
|
Suction & evacuation
|
|
4th pregnancy
|
High initial Beta HCG with no further increase
|
Further evaluation with imaging
|
- Mildly bulky uterus with hypoechoic lesion having multiple vascular channels and cytic spaces with internal vasculairty in the right lateral wall.
- Plain and Contrast enhanced MRI:
- Right lateral wall uterine AVM.
[Fig. 18]
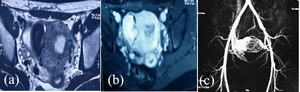
Fig. 18: (a) T2 weighted axial pelvic MRI shows a large signal void on the right lateral uterine wall (b) Intense contrast enhancement is noted in the flow void on axial T1 Weighted fatstat contrast enhanced image.
(c) MR angiogram shows large AVM with a vascular lake communicating with bilateral hypertrophied uterine arteries.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
- Large uterine AVM supplied by bilateral uterine arteries with early venous drainage into internal iliac veins.
The AVM was embolized with glue and PVA particles.[Fig. 19,
Fig. 20]
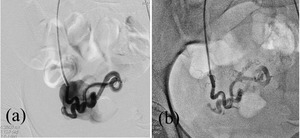
Fig. 19: (a)Right uterine artery angiogram shows hypertrophied right uterine artery branch draining into a large vascular lake. (b) Post embolization check angiogram shows no filling of the vascular lake with reduction of flow in the AVM.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
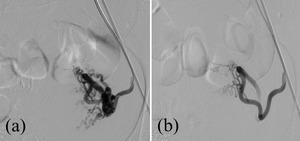
Fig. 20: ( a)Left uterine artery angiogram shows tiny multiple tortuous feeder arteries to the AVM arising from uterine artery (b) Post embolization angiogram shows significantly reduced flow through feeder arteries.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733
- On elective basis,
successful embolization was done in all three patients
- One patient required repeat embolization at the end of one and half months.
- All three patients are currently asymptomatic at the end of one and half years post procedure.

 suggesting glue embolization. References: Agarwal, Neha, et al. "Congenital Uterine Arteriovenous Malformation Presenting as Postcoital bleeding: A Rare Presentation of a Rare Clinical Condition." Journal of clinical imaging science 7 (2017).")
 showing heterogeneous signal intensity focal mass in the antero-inferior uterine wall with blooming on T2* image(b) References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
 and filling of early draining veins.(b) References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
: 4727-4733")
 and post embolisation image showing reduction in supply to the AVM with glue cast in the vessel bed.(b) References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
 Repeat DSA through Right internal iliac artery one and half month later shows no flow to the AVM from the right uterine artery. Note the glue cast from previous embolization within the vessel bed.(b) Selective left uterine artery angiogram demonstrates residual AVM supplied through hypertrophied tortuous left uterine artery branches and early drainage into right internal iliac vein. References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
: 4727-4733")
: 4727-4733")
 demonstrates a large AVM with nidus. (b) Post embolization check angiogram showing significant reduction of flow in the AVM. References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
 Selective Left uterine artery angiogram showing hypertrophied left uterine artery supplying feeder artery branches to the AVM (b) Post embolization check angiogram shows stasis and reduction of flow in the AVM. Also noted is the glue cast in the vessel bed. References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
 T2 weighted axial pelvic MRI shows a large signal void on the right lateral uterine wall (b) Intense contrast enhancement is noted in the flow void on axial T1 Weighted fatstat contrast enhanced image.
(c) MR angiogram shows large AVM with a vascular lake communicating with bilateral hypertrophied uterine arteries.
References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
Right uterine artery angiogram shows hypertrophied right uterine artery branch draining into a large vascular lake. (b) Post embolization check angiogram shows no filling of the vascular lake with reduction of flow in the AVM. References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")
Left uterine artery angiogram shows tiny multiple tortuous feeder arteries to the AVM arising from uterine artery (b) Post embolization angiogram shows significantly reduced flow through feeder arteries. References: Pankar Uma, Indusekhar S., Pannag Desai, & Vidya Bhargavi. "Uterine arteriovenous malformation-beyond surgery: a case series." International Journal of Reproduction, Contraception, Obstetrics and Gynecology [Online], 6.10 (2017): 4727-4733")