The lumbosacral spine is the source of pain,
suffering,
and disability more frequently than anyother part of the body. When low back pain does not improve with conservative management,
the cause of the pain must be determined before further therapy is initiated. After a symptomatic structure has been identified,
therapeutic spinal injections may be administered as an adjunct to conservative management,
especially in patients with inoperable conditions.
ANATOMY
OSSEOUS STRUCTURES
The lumbar vertebra has anterior elements (consisting of the vertebral bodies),
middle elements (consisting of the pedicles),
and posterior elements (consisting of the facet joints,
the lamina,
spinous processes,
and transverse processes).
The anterior elements sustain compressive loads applied to the spine,
whereas the posterior elements control spinal motion through the ligaments and muscles attached to these osseous structures.
The middle elements connect the anterior vertebrae body to the posterior elements,
and transfer loads between these components.
INTERVERTEBRAL DISC
The intervertebral disc is interposed between the vertebral bodies,
and consists of a central gelatinous nucleus pulposis,
a surrounding dense annulus fibrosis,
and the cartilaginous vertebral end plates capping the adjacent vertebral body surfaces.
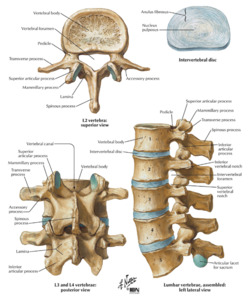
Fig. 1
References: Frank H. Netter. Atlas of Human Anatomy.
LUMBAR LIGAMENTS
The posterior ligaments of the lumbar spine consist of the interspinous,
super-spinous,
and intertransverse ligaments,
which ones are not substantial structures and add little to lumbar spine stabilization.
The ligamentum flavum courses between adjacent lamina,
providing some resistance to flexion and a distinct elastic smooth surface along the dorsal aspect of the vertebral canal.
The posterior longitudinal ligament is a thin and weak ligament that does little to impede separation of the vertebral bodies.
In contrast,
the anterior longitudinal ligament is more robust and significantly resists hyperextension between the vertebral bodies.
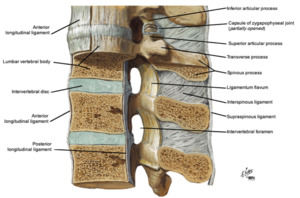
Fig. 2
References: Frank H. Netter. Atlas of Human Anatomy.
LUMBAR MUSCLES AND FASCIA
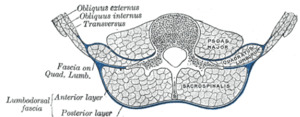
Fig. 3
References: Henry Vandyke Carter-Henry Gray. Anatomy of the Human Body.
NERVE SUPPLY OF THE LUMBAR SPINE
The nerve supply to the lumbar paravertebral muscles is extensive.
Dorsal and ventral nerve roots join to form the spinal nerve,
which subsequently divides into two rami:
- The ventral ramus of the spinal nerve innervates the psoas major,
quadratus lumborum,
and intertransversarii muscles.
- The dorsal ramus of the spinal nerve innervates the posterior lumbar muscles and other structures posterior to the intervertebral foramen.
The dorsal ramus subdivides into three major branches:
- The lateral branches of the dorsal ramus innervate the iliocostalis lumborum muscle.
- The intermediate branches supply the longissimus muscles.
- The medial branches innervate the short multifidus muscle,
inter-spinous ligament,
and the facet joints.
The vertebral bodies are innervated by the gray rami communicantes (from the sympathetic trunk) and the ventral ramus forming the anterior longitudinal and posterior longitudinal plexuses.
The intervertebral discs are innervated by multiple sources: the gray rami communicantes anterolaterally,
the ventral rami posterolaterally,
and the sinuvertebral nerves posteriorly.
The sinuvertebral nerves are recurrent branches of the ventral ramus and supply the posterior longitudinal ligament,
the posterior (dorsal) aspect of the disc,
and the anterior (ventral) aspect of the dura mater.
The posterior (dorsal) aspect of the dura,
however,
has no nerve supply.
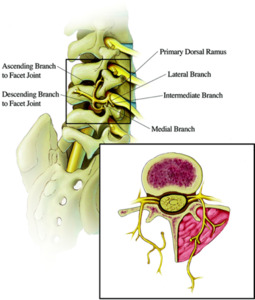
Fig. 4
References: Veizi E. and Hayek S. 2014. Interventional Therapies for Chronic Low Back Pain. Neuromodulation. 17: 31–45
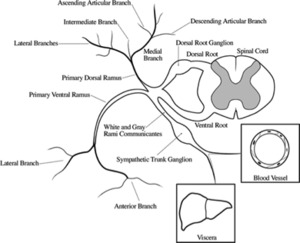
Fig. 5
References: Steven P. Cohen, M.D.; Srinivasa N. Raja, M.D. 2007. Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint Pain. Anesthesiology. 106:591– 614.
POTENTIAL PAIN SOURCES
The vast majority of low-back pain is mechanical in nature and is usually related to spinal degeneration,
or subclinical episodes that are aggravated intermittently by episodes of trauma.
This ‘degenerative cascade’,
as described by Yong-Hing and Kirkaldy-Willis,
produces degenerative joint changes in the articular cartilage of the facet joints,
loss of hydration of the intervertebral disks with concomitant loss of stability and resistance to torsion,
eventually leading to radial tears in the annulus.
These annular tears allow herniation of the disc material out of the disc into the vertebral canal and onto the adjacent nerve root,
causing the symptom of ‘sciatica’ or pain in the distribution of that involved nerve root.
The damaged disc also releases neuropeptide,
phospholipase A2,
and inflammatory peptides,
further irritating the nearby neurological structures.
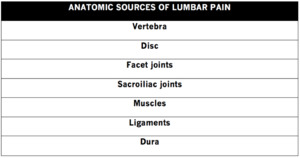
Fig. 6
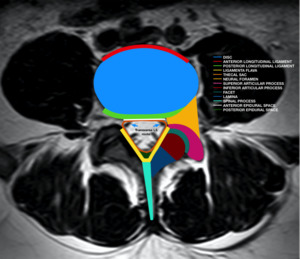
Fig. 7: Sources of pain generators
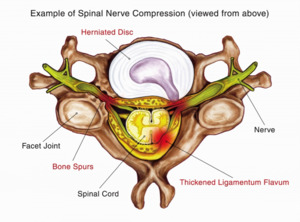
Fig. 8
References: Joshua M. Ammerman. 2018. Spinal Canal, Vertebrae, Facet Joints, and Foramen: How They're Affected by Spinal Stenosis. SpineUniverse Blog.
