IMAGING IN PROCEDURAL SELECTION
Symptom-imaging correlation guides procedural selection and planning.
It enables one to verify the appropriateness of the requested intervention or justify modification.
Procedural selection begins with a judgment on the pain generator.
The symptom-imaging correlation exercise is to interview the patient before we review the MR images,
and then deduce the most likely pain generator and predict the MR imaging findings.
Other variation is reviewing the MR images before the interview of the patient,
so it is posibble to deduce the most likely pain generator and predict the patient’s symptoms.
Symptom-imaging correlations are often obvious,
but surprising mismatches do occur.
In younger patients with acute or subacute radiculopathy,
dermatomal information serves to focus MR image review.
Symptoms usually correlate perfectly with nerve entrapment because of lateralization of single-level disk abnormalities.
Occasionally,
a symptom-specific search will lead to the diagnosis of an intraforaminal or lateral disk extrusion that explains symptoms but that was overlooked at the time of MR image interpretation.
Transforaminal nerve root block (NRB) targets the pain generator and delivers the steroid directly to the inflamed nerve root.
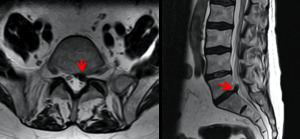
Fig. 9: T2-weighted sagittal and axial MRI showing an extruded disc, compressing the thecal sac para-centrally on the left side at the L5-S1 level and impinging the left S1 nerve root (red arrow).
In older patients with chronic unilateral radiculopathy,
symptom-imaging correlation is more challenging because of multilevel spondylosis.
Transforaminal NRB remains a recommended treatment option if dermatomal information reveals a specific pain generator.
One exception is nerve compression by a facet cyst.
To address this problem,
one can combine percutaneous cyst rupture with intra-articular corticosteroid injection.

Fig. 10: MRI demostrate degenerate facet joints and a large facet cyst from the right L5-S1 facet (red arrow).
In older patients with chronic bilateral radiculopathy,
the radiologist should solicit signs of neurogenic claudication.
One should expect MR imaging to reveal spinal stenosis,
which is the leading reason for spinal surgery.
When MR imaging shows multi-level stenosis,
dermatomal information may indicate the level of pain generator.
Interlaminar epidural steroid injection (ESI) is the recommended procedure because the corticosteroid can spread cranially and caudally over multiple disk levels.
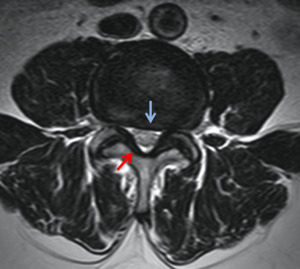
Fig. 11: T2-weighted MRI image through the L3 disc space that demonstrates moderate to severe central stenosis secondary to severe ligamentum flavum thickening (red arrow), facet joint hypertrophy, and disc bulging (blue arrow). In this case, the nerve root compression resulted in patient symptoms of neurogenic claudication.
When symptoms suggest lumbar facet syndrome (posterior ramus syndrome),
one must scrutinize the zygapophyseal joints for signs of inflammation,
including effusion,
capsulitis,
and periarticular edema.
Back pain may radiate into the buttocks,
groin,
or posterior thigh and may worsen with prolonged standing and extension and rotation or lateral bending movements.
If corticosteroid administration alleviates symptoms,
systematic anesthetic injections (medial branch blocks) yield corroborative diagnostic information prior to radiofrequency or quimical ablation.
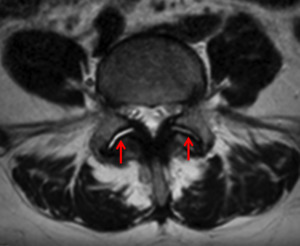
Fig. 12: T2 weighted MRI image showing fluid collection in both facet joints, in relation to facet syndrome.
THERAPEUTIC TECHNIQUES FOR LOW BACK PAIN
EPIDURAL INJECTION
Patient selection for epidural injections is poorly described in the literature.
We have used epidural injections for treatment of local pain or radiculopathy in the settings of documented disk herniation,
central or foraminal stenosis,
and absent imaging findings.
The technique is usually used if rest has failed to relieve the symptoms or if the patient is considered a surgical candidate but does not desire to undergo surgery.
Various combinations of saline solution,
local anesthetics,
and steroids have been injected.
Theories for explaining the method of relief include lysis of adhesions,
change in relationship between the disk and the nerve root,
anesthetic breaking the pain cycle,
and reduction of inflammation and swelling.
Dorsal interlaminar,
sacral hiatus,
and foraminal approaches may be used for lumbosacral epidural injection.
Epidurography with nonionic myelography-approved iodinated contrast material is recommended to document epidural position and evaluate the distribution pattern. The air defines the epidural space as well as contrast material,
confirming appropriate needle placement.
For a dorsal interlaminar approach,
the patient is placed in the prone position.
A 22-gauge spinal needle is advanced to the posterior margin of the spinal canal.
Positioning in the epidural space is detected with a loss-of-resistance technique.
Gentle intermittent pressure is applied on a syringe while advancing the needle.
A sudden loss of resistance occurs on entering the epidural space.
Absence of cerebrospinal fluid flow is verified with aspiration.
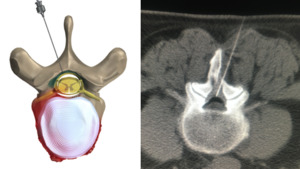
Fig. 13: Interlaminar approach epidural injection
References: Left pic.: Novocur. Right pic.: Hospital Universitario Fundación Jiménez Díaz, Hospital Universitario Fundación Jimenez Díaz - Madrid/ES
For the sacral hiatus,
the patient is placed in the prone position.
The sacral cornua (ie,
the border of the sacral hiatus) and median sacral crest are palpated and localized fluoroscopically.
A 22-gauge spinal needle is advanced via the sacral hiatus into the sacral canal until its tip reaches the S3 level.
Keeping the needle below the S2-3 disk space minimizes the risk of dural puncture.
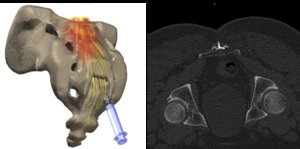
Fig. 14: Caudal approach epidural injection
References: Left pic.: Novocur. Right pic.: Hospital Universitario Fundación Jiménez Díaz, Hospital Universitario Fundación Jimenez Díaz - Madrid/ES
For a lumbar foraminal approach,
the patient is placed in the prone position and a 22-gauge needle is advanced under the pedicle of the appropriate segment,
similar to the approach used for lumbar nerve root injection.
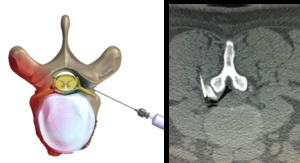
Fig. 15: Transforaminal epidural injection
References: Left pic.: Novocur. Right pic.: Hospital Universitario Fundación Jiménez Díaz, Hospital Universitario Fundación Jimenez Díaz - Madrid/ES
FACET JOINT INJECTION
Facet joint injection may be considered either diagnostic or therapeutic.
CT guidance or fluoroscopic guidance may be used for facet joint injections.
Levels for injection are selected on the basis of local pain or tenderness and imaging evidence of disease.
It is often difficult to localize the pain to one level,
so that generally two and occasionally three levels are injected.
If the pain is bilateral,
injections are performed bilaterally.
There are reports of long-term (3– 6 months) success and failure.
Denervation of the facet joint may also be performed with CT guidance or fluoroscopic guidance.
This procedure has been performed with 95% ethanol or with radio-frequency techniques.
Gangi et al denervate facet joints using CT guidance with 95% ethanol.
Twenty-two-gauge spinal needles are advanced into the internal superior borders of the transverse processes above and below the target facet joint.
One mL of nonionic contrast material is injected to predict ethanol diffusion,
and 1.5 mL of 95% ethanol is injected at each level.
A facet joint is supplied by the nerve exiting at the level of the facet joint as well as at the next higher level.
Denervating a facet joint requires that two rhizotomies be performed.
For example,
denervation of the right L3-4 facet joint requires rhizotomy of right L2 and L3.
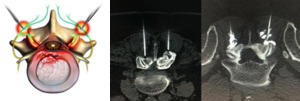
Fig. 16: Bilateral L3-L4 rhizotomy with etanol. In the image on the right, a contrast is injected to predict the distribution volume of etanol.
References: Left pic.: Nucleus Medical Art, Inc.. Right pic.: Hospital Universitario Fundación Jiménez Díaz, Hospital Universitario Fundación Jimenez Díaz - Madrid/ES
SELECTIVE NERVE ROOT INJECTION
Nerve root injection is indicated in patients with radicular symptoms; acute diskogenic symptoms without nerve paralysis that is resistant to conventional medical therapy; and post-diskectomy síndrome.
Inflammation of the nerve root is presumed to be the cause of the pain.
In a study by Zennaro et al,
selective nerve root injection provided pain relief in 70% of all patients and in 95% of patients with foraminal stenosis secondary to degenerative stenosis rather than disk herniation.
These authors used CT guidance and injected 0.8 mL of 1% lidocaine with 75 mg of hydrocortisone.
Selective nerve root injections often result in a degree of epidural injection,
which may play a role in pain relief.
Typically,
injection is performed at a single level that correlates with the radiculopathy.
For selective lumbar nerve root injections,
the area of interest is scanned with the patient in the prone position.
Transligamentary ans approaches may be used for nerve root injection.
The skin entry site and the angle of approach are determined,
and a 22-gauge needle is advanced adjacent to the exiting nerve root.
Patients usually report reproduction of pain along the distribution of the nerve.
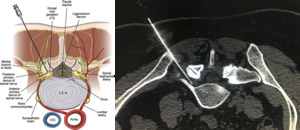
Fig. 17: Right L5 tranforaminal nerve root injection
References: Left pic.: James P. Rathmell et al. 2015. Safeguards to Prevent Neurologic Complications after Epidural Steroid Injections Consensus Opinions from a Multidisciplinary Working Group and National Organizations. Anesthesiology. 122:974–84. Right pic.: Hospital Universitario Fundación Jiménez Díaz, Hospital Universitario Fundación Jimenez Díaz - Madrid/ES
SACROILIAC JOINT INJECTION
The indications for sacroiliac joint injection are acute or chronic sacroiliac joint pain that is not adequately controlled with nonsteroidal anti-inflammatory agents.
The procedure is frequently performed in patients with seronegative inflammatory sacroiliitis.
With CT guidance,
the middle third of the joint is usually most accessible and is accessed with a dorsal angulated approach.
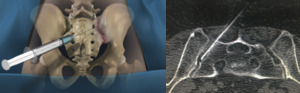
Fig. 18: Left sacroiliac joint injection
References: Left pic.: Los Angeles Minimally Invasive Spine Institute. Right pic.: Hospital Universitario Fundación Jiménez Díaz, Hospital Universitario Fundación Jimenez Díaz - Madrid/ES
DECOMPRESSION OF SYNOVIAL CYSTS
Synovial cysts have been associated with radicular and claudication symptoms,
based on their location,
size,
and compression of adjacent structures.
These lesions can be easily accessed percutaneously with imaging guidance of the needle into the facet joint,
though direct puncture of cysts via a sublaminar approach can also be performed.
Given the concomitant osteoarthritic changes,
CT guidance is often preferred over fluoroscopy to access the joint.
A mixture of steroid,
anesthetic,
and contrast is injected into the joint space,
with the goal of rapid expansion resulting in cyst rupture.
Success is confirmed by epidural spread of contrast.
Serial reports have confirmed the efficacy of this therapy,
which may delay or obviate surgical resection of the cysts.
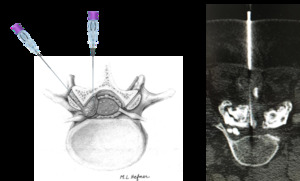
Fig. 19: Right L4-L5 synovial facet cyst descompression.
References: Left pic.: M.L.Hefner. Right pic.: Hospital Universitario Fundación Jiménez Díaz, Hospital Universitario Fundación Jimenez Díaz - Madrid/ES
