The use of filling materials for soft tissue augmentation dates from the late 19th century.
Since its discovery,
silicone has been used for multiple medical-aesthetic purposes.
It was prepared in different degrees of density,
from liquid to solid.
Due to the immediate and delayed complications that occurred,
autologous fat was used to fill wrinkles or depressions,
and little by little other types of materials such as collagen,
calcium hydroxyapatitia,
hyaluronic acid,
etc,
were included.
Cosmetic fillers (CF) are principally used to treat wrinkles and sagging skin.
According to data of the American Society for Aesthetic Plastic Surgery,
there has been a 279% increase in the total number of cosmetic procedures since 1997,
and an increased in derived complications as well.
In 2013,
around 9.5 million non-surgical cosmetic procedures were performed.
The injection of hyaluronic acid is the second most common non-surgical cosmetic procedure being the face the most frequent injection site for this type of cosmetic agents (Fig. 2).
Fig. 2: Introduction
Ultrasound (US),
preferably,
High Resolution Ultrasound (HRUS),
is considered the gold standard for evaluation of cutaneous foreign materials.
It is able to detect and identify the most common types of cosmetic fillers.
CF can be divided depending on their composition,
depending on their form of presentation (gel,
liquid,
gelatin) or depending on the skin layer in which they are being injected (intradermal or subcutaneous). They can also be biologicals and synthetics depending on the source used for their creation. However for dermatologists or for practical purposes it is more useful to use the classification according to their permanence (Fig. 3).
So,
CF are widely classified into:
- Non-permanent
- Semi-permanent
- Permanent
| Classification |
Permanence |
e.g. |
| Non-permanent |
4-8 months (Biodegradable) |
Hyaluronic acid,
Collagen,
Agarose and autologous fat. |
| Semi-permanent |
12-18 months |
Calcium hydroxyapatita,
polylactic acid, and polycaprolactone. |
| Permanent |
No time limit (Non- biodegradable) |
Polymethylmethacrylates (PMMA),
Silicone and Polyacrylamides, |
Table 1. Classification of CF.
In general,
there is a more generic classification which is being used in daily practice: Resorbable and non-resorbable.
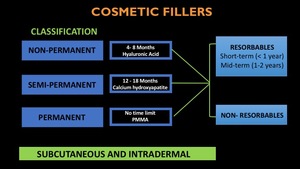
Fig. 3: CF classification
ANATOMY OF NORMAL SKIN
Skin is the largest and most superficial organ in human beings. It is a very complex organ,
both histologically and functionally,
which has a wide range of active,
as well as passive functions,
incuding:
- Protective coating
- Photosynthesis of vitamin D3
- Regulatation of body temperature
- Communication between internal bodies and external agents.
Skin diseases are usually expressed with a specific distribution (pattern) that reflects the non-homogeneity of the blood supply and nerves.
Occasionally primary alterations of superficial structures can simulate dermal pathology.
Therefore,
It is important to know both the morphology of the skin and the adjacent surface structures (Fig. 4).
There are mainly two different types of skin:
- Thick skin - Hairless (found in palms and soles)
- Thin skin - Hairy
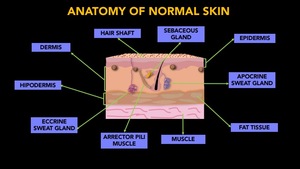
Fig. 4: Anatomy of normal skin
Skin is composed of three primary layers:
| Layer |
Characteristics |
Components |
| Epidermis |
The most superficial.
Highly cellular and non-vascular.
keratinocytes,
melanocytes,
Langerhans cells and Merkel cells.
|
Appendages:
- Hair follicle
- Nails
- Sweat glands.
- Pilosebaceous unit: epidermal invagination that contains the hair follicle,
sebaceous gland and the erector hair muscle.
Layers:
- Stratum Corneum
- Stratum Lucidum
- Stratum Granulosum
- Stratum Spinosum
- Stratum Basale
|
| Dermis |
Support structure with mechanical functions.
Complex vascular system: Superficial plexus,
arteriovenous anastomoses and
glomus bodies.
Cells (fibroblast and mast cells),
collagen ,
elastic fibers,
glycosaminoglycans and glycoproteins.
|
Appendages:
- Blood vessels
- Lymphatics.
- Nerve fibers.
- Deep part of the hair follicles.
- Sweat glands.
Layers:
- Superficial - Papillary
- Deep - Reticular
|
| Hipodermis - subcutaneous tissue |
Subcutaneous adipose tissue compartment divided into lobules
Fat cells and separated by fibrovascular septa.
Collagen and reticular fibers
|
Appendages:
- Blood vessels
- Lymphatics.
- Nerves
|
Table 2. Skin layers.
ULTRASOUND OF THE SKIN
The skin is very easy to access by US,
considering US as the gold standard for its assesment.
However,
HRUS is preferred. Different layers named above can be differentiated and evaluated separately by HRUS (Fig. 5).
Furthermore,
there are some technical considerations,
including:
- Multichannel US - High frequency transducers >/= 15 MHz.
- Hockey stick or foot print transducers
- Surface couplers (gel pad) or abundant US transmission gel
- Gray scale and color Doppler
- Panoramic acquisitions
- Operator skills and expertise - operator dependant.
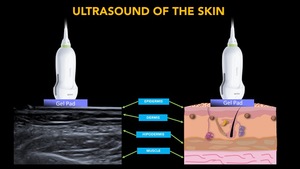
Fig. 5: Anatomy of normal skin and its representation on ultrasound.
Epidermis:
Fig. 6
- Epidermal keratin is highly ecogenic
- Highly keratinized segments (palms and soles) show an hyperechogenic bilaminar structure.
- Low keratinized segments have a simple hyperechoic laminar appearance.
Dermis:
Fig. 6
- Echogenicity depends on the amount of collagen
- You will see some hyperechogenic bands.
- Subepidermal hypoechoic band (Fig. 7).
- It is rarely possible to detect blood flow on color Doppler in a normal dermis.
If it is very evident,
look for pathology.
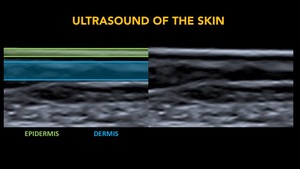
Fig. 6: Ultrasound of the skin. Epidermis and Dermis.
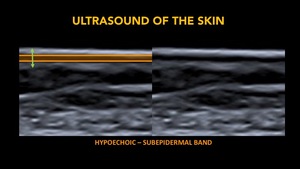
Fig. 7: Subepidermal band.
Hypoechogenic band that lies below the epidermis, defined by De Rigal et al in 1989.
The thickness of this band increases with age, being used as an aging marker
It reflects structural alterations of the skin and water accumulation in the papillary dermis.
The total thickness is the perpendicular distance from the epidermis (including it) to the deepest point of the dermal band, which is a hyperechoic band. It is also call, dermo-hypodermic junction, and always regardless of its echogenicity will mark the border with the hypodermis.
Hipodermis:
- Hypoechogenic fatty lobules with hyperechogenic fibrous septa.
- Subcutaneous circulation can be visualized on color Doppler as a low-flow pattern.
THIRDS OF THE FACE
Superior Third:
- It goes from the supraorbital rim to the anterior hair line.
- Areas to asses: Temporal,
Forehead,
Eyebrows,
Upper eyelid and glabella.
- It is the least involved in the use of CF.
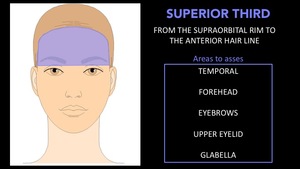
Fig. 8: Horizontal thirds of the face. Superior Third.
Middle Third:
- It goes from the supraorbital rim to the nasal base.
- Areas to asses: Cheeks,
Lower eyelid,
Lateral periorbital lines and nose.
- It is the the second most involved in the use of CF.
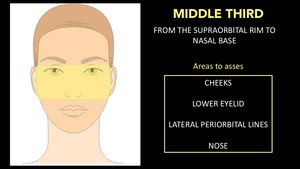
Fig. 9: Horizontal thirds of the face. Middle Third.
Inferior Third:
- It goes from the nasal base to the menton.
- Areas to asses: Chin,
Jawlines,
Nasolabial folds and Marionette lines.
- It is the the most involved in the use of CF.
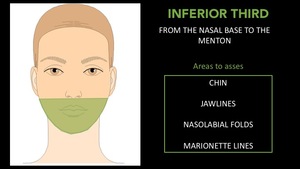
Fig. 10: Horizontal thirds of the face. Inferior Third.
FACE MAPPING
Face mapping (FM) emerged at our hospital as a need for better communication between radiologists and clinicians.
Especially,
those involve in the cosmetic procedures area,
such us dermatologist,
plastic surgeons and some aesthetic doctors.
FM is based on the horizontal thirds of the face showed above.
It allows radiologist and clinicians to communicate the localization of cosmetic fillers,
as well of its nature - Resorbable Vs Non resorbable (Fig. 11)
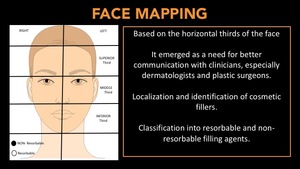
Fig. 11: Face mapping based on the horizontal thirds of the face.
We have designed a map of the face,
in which we demonstrate face thirds,
sides - rigth or left-,
as well as the type of filler (black dot for non-resorbables and white dot for resorbables).
(Fig. 12).
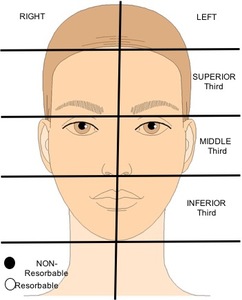
Fig. 12: Face mapping.






 to the deepest point of the dermal band, which is a hyperechoic band. It is also call, dermo-hypodermic junction, and always regardless of its echogenicity will mark the border with the hypodermis.")




