ECR 2019 / C-2688
High Resolution Cutaneous Ultrasound of the Face in the Assessment of Dermal/Hypodermal Cosmetic Fillers
Congress:
ECR 2019
Poster Number:
C-2688
Type:
Educational Exhibit
Keywords:
Foreign bodies, Treatment effects, Ultrasound-Power Doppler, Ultrasound-Colour Doppler, Ultrasound, Soft tissues / Skin, Head and neck
Authors:
L. Brun, G. PALAZUELOS, H. Rivera; Bogota/CO
DOI:
10.26044/ecr2019/C-2688

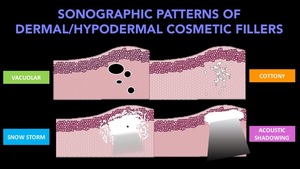
Fig. 13:
Sonographic patterns of dermal/hypodermal cosmetic fillers
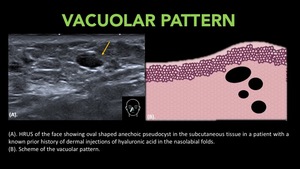
. HRUS of the face showing oval shaped anechoic pseudocyst in the subcutaneous tissue in a patient with a known prior history of dermal injections of hyaluronic acid in the nasolabial folds.
(B). Scheme of the vacuolar pattern.")
Fig. 14:
Vacuolar Pattern
(A). HRUS of the face showing oval shaped anechoic pseudocyst...
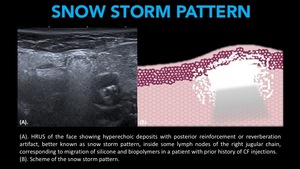
. HRUS of the face showing hyperechoic deposits with posterior reinforcement or reverberation artifact, better known as snow storm pattern, inside some lymph nodes of the right jugular chain, corresponding to migration of silicone and biopolymers in a patient with prior history of CF injections.
(B). Scheme of the snow storm pattern.")
Fig. 15:
Snow Storm Pattern.
(A). HRUS of the face showing hyperechoic deposits with...
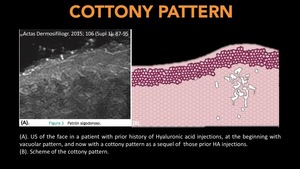
. US of the face in a patient with prior history of Hyaluronic acid injections, at the beginning with vacuolar pattern, and now with a cottony pattern as a sequel of those prior HA injections.
(B). Scheme of the cottony pattern.
References: Actas Dermosifiliogr. 2015; 106 (Supl 1): 87-95")
Fig. 16:
Cottony Pattern.
(A). US of the face in a patient with prior history of...
. HRUS of the face showing hyperechoic deposits with posterior acoustic shadowing, corresponding to a filling agent in a patient with prior history of calcium hydroxyapatite injections.
(B). Scheme of the acoustic shadowing pattern.")
Fig. 17:
Acoustic Shadowing Pattern.
(A). HRUS of the face showing hyperechoic deposits...
. HRUS of the face showing a mixed pattern in a patient with prior history of biological and synthetic cosmetic fillers injections. Snow storm pattern (white arrow) and pseudocysts with mild posterior enhancement due to vacuolar pattern (blue arrow).
(B). Scheme of both patterns.")
Fig. 18:
Mixed Pattern. Snow storm and vacuolar.
(A). HRUS of the face showing a mixed...
. Clinical picture of the patient (permission given).
(B) And (C). HRUS. Round shaped anechoic pseudocyst localized on both jawlines corresponding to hyaluronic acid injections.
(D) And (E). HRUS. Right nasolabial fold, corresponding to the site of patient’s complaint, showing an hyperechoic oval shaped “lesion” with some areas of posterior reverberation artifact (snow storm) and other areas os posterior acoustic shadowing (mixed pattern) corresponding to non-absorbable filling agent.")
Fig. 19:
(A). Clinical picture of the patient (permission given).
(B) And (C). HRUS....
. Clinical picture of the patient (permission given).
(B). Power Doppler ultrasound showing increased blood flow surrounding the lesion due to inflammatory changes.
(C) and (D) longitudinal view HRUS. Comparison of normal and abnormal dermal tissue in a patient with recent history of hyaluronic acid + vitamins dermal injections on both cheeks. Some hypoechoic pseudocysts with inner echoes due to debris associated to increased in echogenicity of surrounding tissue.")
Fig. 21:
(A). Clinical picture of the patient (permission given).
(B). Power Doppler...
. Clinical picture of the patient (permission given).
(B), (C) and (D). HRUS. Mid-Forehead, corresponding to the site of patient’s complaint showing some small nodules (arrows) indicative of hyperechoic deposits of a filling agent with snow storm pattern.")
Fig. 23:
(A). Clinical picture of the patient (permission given).
(B), (C) and (D)....
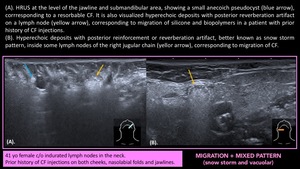
. HRUS at the level of the jawline and submandibular area, showing a small anecoich pseudocyst (blue arrow), corrresponding to a resorbable CF. It is also visualized hyperechoic deposits with posterior reverberation artifact on a lymph node (yellow arrow), corresponding to migration of silicone and biopolymers in a patient with prior history of CF injections.
(B). Hyperechoic deposits with posterior reinforcement or reverberation artifact, better known as snow storm pattern, inside some lymph nodes of the right jugular chain (yellor arrow), corresponding to migration of CF.")
Fig. 24:
(A). HRUS at the level of the jawline and submandibular area, showing a small...
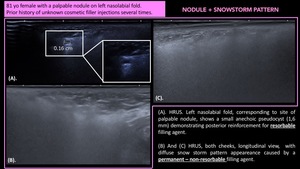
. HRUS. Left nasolabial fold, corresponding to site of palpable nodule, shows a small anechoic pseudocyst (1,6 mm) demonstrating posterior reinforcement for resorbable filling agent.
(B) And (C) HRUS, both cheeks, longitudinal view, with diffuse snow storm pattern appeareance caused by a permanent – non-resorbable filling agent.")
Fig. 20:
(A). HRUS. Left nasolabial fold, corresponding to site of palpable nodule,...
. Clinical picture of the patient (permission given). Photos of the patient in three different episodes of the disease. The US was performed at the time of the first photo from left to right.
(B). Right nasolabial fold. Cottony pattern as as sequel of hyaluronic acid injections.
(C). Right cheek. Diffuse alteration of soft tissues on right cheek and nasolabial fold visualizing some milimetric pseudocyst corresponding to resorbable filling agent, and some areas of snow storm artifact indicative of non-resorbable agent.
(D) Comparison between both nasolabial folds and marionette lines, showing diffuse snow storm pattern, with a small pseudocyst on the left side.")
Fig. 22:
Recurrent Severe Inflammatory Reaction
(A). Clinical picture of the patient...