To learn to appreciate the presence of pathological air,
we must first learn to recognize the physiological air, especially that found in the gastrointestinal tract and in the lung parenchyma.
(Fig. 3)
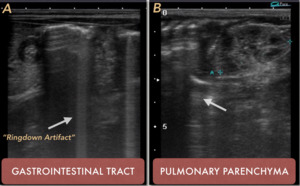
Fig. 3: PHYSIOLOGICAL AIR. Presence of normal distribution air. A. Gastrointestinal tract. B Pulmonary parenchyma. Arrows show the Ringdown Artifact
However,
the pathological air can be found in different regions,
therefore,
its search and study should focus on clinical suspicion.
PATHOLOGICAL DISTRIBUTION OF AIR: (Fig. 4)
⇒ Intra-abdominal
⇒ Retro-peritoneal
- Intraluminal air in preformed structures.
- The air of intraparenchymal location.
- Intramural air
- Soft tissue free air.
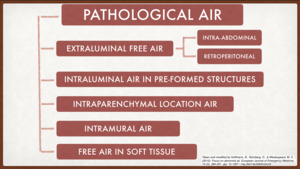
Fig. 4: PATHOLOGICAL AIR. Classification according to location.
Taken and modified of Hoffmann (2012).
References: Taken and modified of Hoffmann, B., Nürnberg, D., & Westergaard, M. C. (2012). Focus on abnormal air. European Journal of Emergency Medicine, 19 (5), 284-291.
EXTRALUMINAL FREE AIR
The presence of extraluminal free air may be a chance finding in some circumstances in relation to the recent history of the procedure (laparotomy,
laparoscopy,
percutaneous biopsy,
peritoneal dialysis or paracentesis).
It is important to know that your presence can last up to 18 days after the procedure(6).
The study,
in this case,
should be customized for each patient,
according to the procedure,
clinical and diagnostic suspicion.
In the case of the study of non-post-procedural pneumoperitoneum,
it should be evaluated based on the suspicion of rupture of the hollow viscera,
peritonitis by gas-forming microorganisms,
rupture of an intra-abdominal abscess, cardiopulmonary resuscitation,
mechanical ventilation or simply by extension of the pneumomediastinum.
and pneumothorax (Macklin Effect).
Highlights among the most important studies on this subject,
the Seitz and Reising (4),
made 30 years ago,
which identifies small quantities as 1 cc.
of free air,
found more frequently in front of the liver and in the left semi-lateral decubitus position,
also describes the displacement of the air when the patient is repositioned.
Muradeli (7) reinforces this theory with the description of the phenomenon ‘Enhanced Peritoneal Stripe Sign (EPSS)’ that consists of the presence of an echogenic,
simple or double superficial line that marks the top of the abdominal wall with the peritoneal content.
Most of the time this finding is associated with later dirty acoustic shadow and reflection artifact generated by the Ringdown artifact. (Fig. 5)
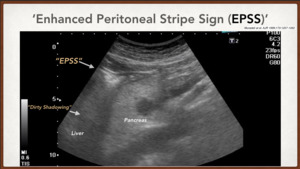
Fig. 5: Enhanced Peritoneal Stripe Sign (EPPS). Muradeli at el. On sonography, enhancement of the peritoneal stripe alone or with reflection artifacts involving the peritoneal stripe is an accurate sign of pneumoperitoneum.
Karahan (11) also provides the "Maneuver of the scissors",
which consists of compressing the caudal part of the probe,
in a parasagittal position on the epigastric line,
displacing the free air represented by the Ringdown artifact towards the sides,
with the objective to decrease the reverberance on the liver; while decompressing the caudal part,
the return of free air to the epigastric region is observed,
accentuating the artifact in ringdown over the liver. (Fig. 6)

Fig. 6: THE MANEUVER OF THE SCISSORS. Taken and modified Karahan, OI, Kurt, A., Yikilmaz, A., y Kahriman, G. (2004).
References: Taken and modified Karahan, OI, Kurt, A., Yikilmaz, A., y Kahriman, G. (2004). New Method for the Detection of Intraperitoneal Free Air by Sonography: Scissors Maneuver. Journal of Clinical Ultrasound,
Ultrasonographic technique for the study of the Pneumoperitoneum
- Most authors suggest the study with the use of high-frequency linear probes to better visualize the superficial peritoneal layer.
- It is also established that the best site for the initial search of the pneumoperitoneum is the right hypochondrium,
superficial to the liver (10),
with the patient in the supine position with the thorax slightly elevated or in the left semi-lateral decubitus position (4,
7,
8,
9).
- The presence of the sign of the ‘Enhanced Peritoneal Stripe Sign (EPSS)’must be sought and,
at the same time,
the "maneuver of the scissors" can be used to check the mobility of the peritoneal free air.
"Pitfalls"
Chilaiditi sign: A rare condition in which the colon gets between the liver and the diaphragm.
Its potential to mimic open air under the diaphragm is well known,
especially in the chest x-ray.
(Fig. 7)
Solution: The dynamic nature of ultrasonography is useful in this situation.
The patient's movement should show that there is no mobile free air in the peritoneum. Also,
prolonged exploration could expose the usual intestinal peristalsis in the anterior hepato-diaphragmatic space.
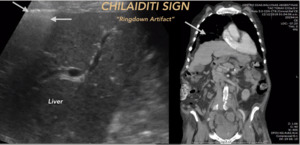
Fig. 7: CHILAIDITI SIGN. A rare condition in which the colon gets between the liver and the diaphragm.
Overlying rib: Can simulate a reverberation artifact suggestive of pneumoperitoneum.
(Fig. 8)
Solution: The origin of the artifact must be traceable to a superficial point to the peritoneal ray and must change with the position of the probe and the patient's movement.
Pulmonary Ringdown Artifact: This artifact can be recognized,
coming from air in the lungs.
During inspiration,
these artifacts may overlap with the reverberations of pneumoperitoneum.
()
Solution: Expiratory examination will show the thoracic and intra-abdominal origins separated from the artifacts.
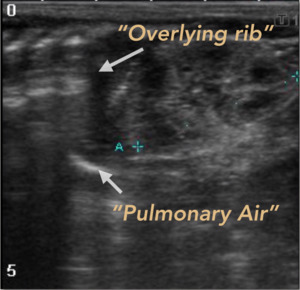
Fig. 8: Pitfalls of the extraluminal free air. The overlying rib and the ringdown artifact generated by the pulmonary alveolar air, can generate frequent errors in the interpretation.
INTRALUMINAL AIR IN PRE-FORMED STRUCTURES
It can be observed inside the bile ducts or the gallbladder,
the venous portal system,
abdominal arteries,
and veins,
inside the bladder and the urogenital tract,
even inside the pancreatic ducts.
The interpretation of the results will depend on the clinical presentation and the circumstances. The two most common causes seem to be a trauma (including iatrogenic manipulation) and infectious ones(12).
Pneumobilia (air in the biliary system)(Fig. 9),
for example,
can be caused by papillotomy,
fistulas within the gastrointestinal tract,
tumor invasion,
or by ascending biliary infection with gas-producing organisms.
The presence of air within the arteries and veins can cause iatrogenic vascular manipulations such as cardiac catheter placement or hemodialysis.
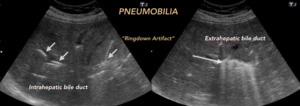
Fig. 9: PNEUMOBILIA. Characterized by the presence of air in the bile ducts, central distribution. Its presence must be analyzed with the previous records and clinical context of the patient.
Pneumoporta is associated with significant mortality,
frequently derived from intestinal necrosis or thrombosis of the mesenteric artery or veins (12).
(Fig. 10)
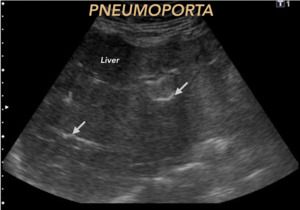
Fig. 10: PNEUMOPORTA. Characterized by the presence of air in the portal venous system, of peripheral distribution. Its presence can alert urgently vital pathology. Arrows mark the presence of intraluminal free air

Fig. 11: HEMATOMETRA. With the presence of air bubbles inside, represented by the Ringdown Artifact, which can mean infection (Endometritis) if there is no traumatic or procedural previous record..
Ultrasonographic technique for the detection of air in preformed structures
- The technique used is similar to that used when evaluating the preformed lumens,
they are those used in the usual abdominal ultrasonography,
with the use of curved probes.
"Pitfalls"
Multiple biliary hamartomatosis: Observed as the presence of multiple hyperechoic foci that generate artifact the ´comet-tail´ in the bile duct,
which could be confused with the presence of Neumobilia or Pneumoporta.
(Fig. 12)
Solution: An important factor is a differentiation between the ´comet-tail´ artifact of the hamartomatosis and the Ringdown artifact by the presence of air.
The latter maintains the width of the artifact in the depth.
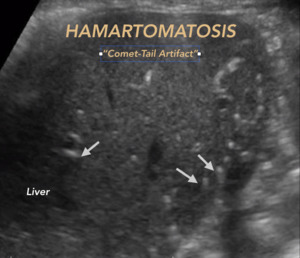
Fig. 12: BILIARY HAMARTOMATOSIS. Pitfall. Multiple hyperechoic foci that generate comet-tail artifact in the bile duct.
INTRA-PARENCHYMAL LOCATION AIR
Among the causes for this finding are an infection and abscess formation (Fig. 13,
Fig. 14,
Fig. 15).
Trauma (including iatrogenic) or neoplasm when they erode in the solid tissue that contains air.

Fig. 13: LIVER ABSCESS. Male 65 years old. Liquid formation with air bubbles inside that generate Ringdown artifact.
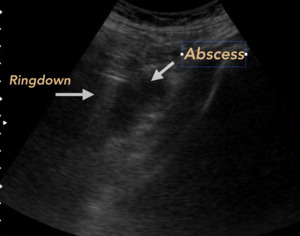
Fig. 14: ABSCESS OF PSOAS. Male 55 years old, diabetic. It is recognized liquid collection located in psoas muscle, associated with air bubbles that generate Ringdown Artifact.
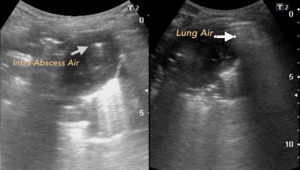
Fig. 15: LUNG ABSCESS. Child of 3 years with cough and fever of 3 weeks of evolution. Gray arrow points to the air inside the Abscess. White arrow indicates pulmonary alveolar physiological air.
Ultrasound technique for the detection of intraparenchymal free air
- The technique used is similar to that used to evaluate the solid organs used in routine abdominal ultrasonography,
with the use of curved probes and the necessary position changes with respect to the organ to be evaluated.
- However,
given the circumstances,
high-frequency linear probes can be used in a complementary manner,
depending on the site of interest and its proximity to the cutaneous surface.
INTRAMURAL AIR
When the presence of air bubbles represented by the artifact in Ringdown is in the thickness of the vesicular wall (emphysematous cholecystitis)(Fig. 16),
the intestinal wall (intestinal pneumatosis) and in the bladder wall (emphysematous cystitis),
it is usually related to infection,
ischemia,
and trauma; it usually involves an emergency diagnosis.
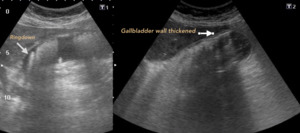
Fig. 16: EMPHYSEMATOUS CHOLECYSTITIS. The presence of air bubbles that generate Ringdown artifact in the thickened anterior wall of the gallbladder is observed.
Ultrasonic technique for the detection of intramural air
- The challenge is focused on the adequate evaluation of the walls of the structure of interest so that the probe to be used should be a linear high frequency.
- The ultrasound beam must be aligned perpendicular to the light of the structure,
to try to overcome the dirty shadow that generates the artifact in Ringdown and avoid errors of appreciation.
"Pitfalls"
Pseudoneumatosis: The intraluminal air bubbles can be falsely projected into the layers of the wall,
this due to the tangential effects.
This artifact can also be visualized in areas of the intestine in which gas bubbles can be trapped in prominent intestinal folds.
Solution: The location of the air should change from intramural to intraluminal with the angulation of the probe.
Also,
there is no evidence of the ringdown artifact in the lower part of the intestinal wall.
Gallbladder Adenomyomatosis: benign leiomyomatous proliferative neoformations of the superficial epithelium of the wall,
characterized by the presence of punctate echogenic images that generate artifact in comet tail.
(Fig. 17)
Solution: It is essential to distinguish the Comet-tail artifact (short tail and a steady decrease in width) and the Ringdown artifact (long and persistent width tail).
As well as the context and degree of clinical suspicion.
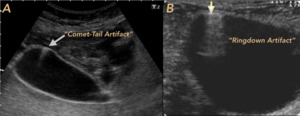
Fig. 17: PITFALLS. A. BILIAR VESICULAR ADENOMYOMATOSIS. Artifact in comet tail is recognized. B. PSEUDONEUMATOSIS IN BLADDER. It turned out to be intraluminal free air secondary to bladder catheter placement.
FREE AIR IN SOFT TISSUES
Special situations are identified in which it is possible to observe the presence of air collections,
represented by the Ringdown Artifact in the subcutaneous cellular tissue,
without traumatic previous record and that by itself,
could indicate the presence of urgency,
in some cases "vital".
For example,
the presence of air in the subcutaneous cellular tissue perineal,
perianal and genital regions could indicate the presence of necrotizing fasciitis (Fournier's gangrene) (13) in which rapid diagnosis is essential to facilitate immediate surgical debridement because the Sequential progression of tissue necrosis can reach 2 to 3 cm per hour.
(Fig. 18)
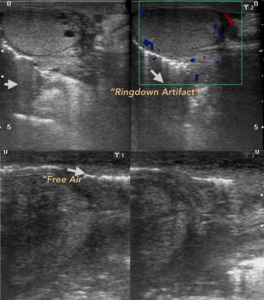
Fig. 18: FOURNIER GANGRENE. Male, 65 years old, with crepitant lesions in the perineal and genital region. Presence of multiple air bubbles, some generate Ringdown artifact
Another entity,
in particular,
is the dermal/subdermal infection by gas-forming microorganisms in which the presence of air bubbles in the subcutaneous cellular tissue is detected,
without a traumatic previous record or the presence of communication with the cutaneous surface.
The main agent is S.
Pyogenes.
(Fig. 19)

Fig. 19: FREE AIR IN SOFT TISSUES. Their finding should alert the radiologist to the presence of dermal / subdermal infections.
Ultrasonographic technique for the detection of air in soft tissues
- As with most soft tissue scans,
it is convenient to use a high-frequency linear probe.
- The presence of air bubbles,
represented by the Ringdown Artifact,
should immediately alert the examiner and the possible causes should be analyzed.
"Pitfalls"
Communication with the cutaneous surface: Beware! When identifying the presence of air bubbles in the subcutaneous cellular tissue and issuing a hurried diagnosis, it is important to rule out the communication of the area of interest with the cutaneous surface,
this being the origin of the entrance of the air bubbles.
Solution: Discard skin lesions that may eventually be communicated with the site of the finding.


. References: Taken and modified of Hoffmann, B., Nürnberg, D., & Westergaard, M. C. (2012). Focus on abnormal air. European Journal of Emergency Medicine, 19 (5), 284-291.")
. Muradeli at el. On sonography, enhancement of the peritoneal stripe alone or with reflection artifacts involving the peritoneal stripe is an accurate sign of pneumoperitoneum.")
.
References: Taken and modified Karahan, OI, Kurt, A., Yikilmaz, A., y Kahriman, G. (2004). New Method for the Detection of Intraperitoneal Free Air by Sonography: Scissors Maneuver. Journal of Clinical Ultrasound,")




 if there is no traumatic or procedural previous record..")






