ECR 2019 / C-2759
Pleural endometriosis: when to suspect?
Congress:
ECR 2019
Poster Number:
C-2759
Type:
Educational Exhibit
Keywords:
Education and training, Diagnostic procedure, MR, CT, Conventional radiography, Thorax, Respiratory system
Authors:
C. S. Kiebert1, G. O. R. D. Rego1, Y. C. S. Neves2, D. Y. Otto1, L. P. Teixeira1, T. L. Matuki1, R. Guerrini1, M. V. Y. Sawamura1; 1São Paulo/BR, 2Salvador, Ba/BR
DOI:
10.26044/ecr2019/C-2759
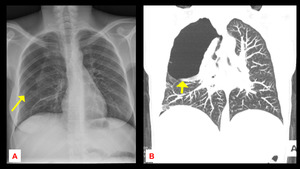
 and coronal chest CT scan (B) demonstrate a right sided pneumothorax.")
Fig. 3:
Case 1: Catamenial pneumothorax. CR (A) and coronal chest CT scan (B)...

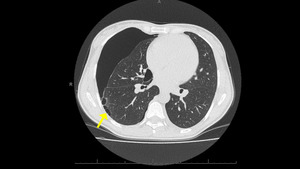
Fig. 4:
Case 1: Catamenial pneumothorax. Axial chest CT scan demonstrates a right sided...

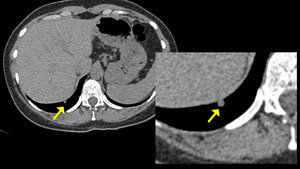
Fig. 5:
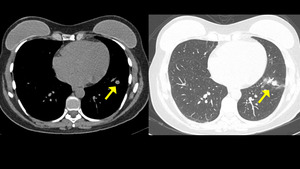
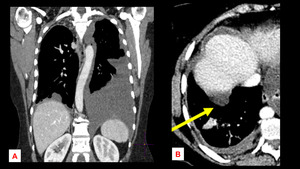
Case 2: Nodular pleural thickening implant adjacent to the diaphragm. Axial...

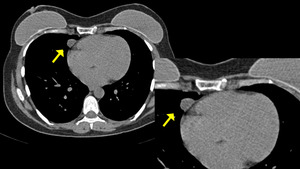
Fig. 6:
Case 2: Nodular pleural thickening implant adjacent to the mediastinum. Axial...
. References: Hospital Sírio Libanês - São Paulo/ Brazil")
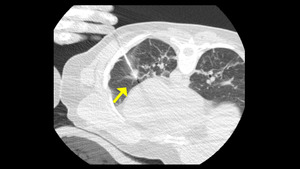
Fig. 7:
Case 2: Axial CT images show an intrapulmonary nodule (arrow).

Fig. 8:
Case 2: CT – guided percutaneous biopsy of left lung nodule.
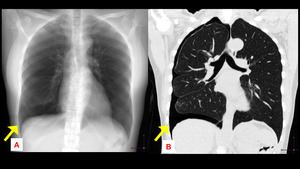
 and coronal chest CT scan (B) demonstrate a partial pulmonary collapse and right sided pneumothorax.")
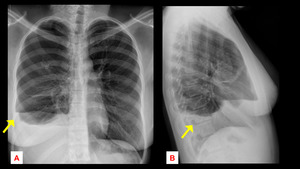
Fig. 9:
Case 3: Catamenial pneumothorax. CR(A) and coronal chest CT scan (B)...
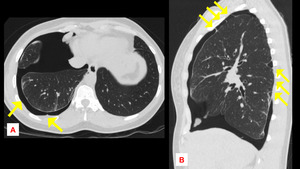
 and sagittal (B) CT images show right-sided pneumothorax and pleural adhesion (arrows).")
Fig. 10:
Case 3: Catamenial pneumothorax. Axial (A) and sagittal (B) CT images show...

Fig. 11:
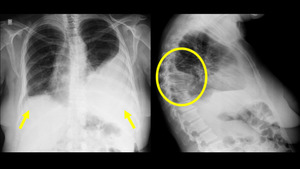
Case 4: Catamenial hemomothorax. CR images demonstrate bilateral pleural...
. Axial CT image shows a nonspecific nodular pleural thickening (B).")
Fig. 12:
Case 4: Catamenial hemomothorax. Coronal CT image demonstrates bilateral...
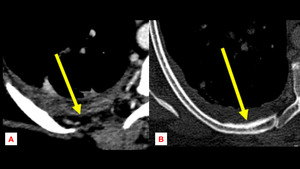
 and inner cortical thickening of of adjacent rib (B), suggesting chronicity.")
Fig. 13:
Case 4: Catamenial hemomothorax. Axial CT images show an extrapleural fat...

Fig. 14:
Case 5: Catamenial hemopneumothorax. CR images demonstrate right-sided...
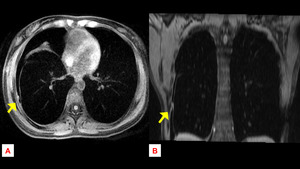
 and coronal (B) T1WI show high signal-intensity nodule (arrows) attached to the parietal pleura surface.")
Fig. 15:
Case 5: Catamenial hemopneumothorax. Axial (A) and coronal (B) T1WI show high...
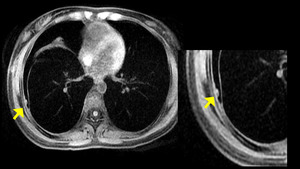
 attached to the right parietal pleura surface.")
Fig. 16:
Case 5: Catamenial hemopneumothorax. Axial T1WI shows high signal-intensity...
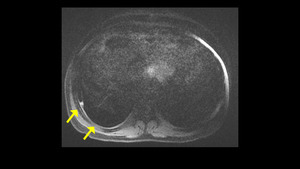
, suggestive of hemorrhagic content.")
Fig. 17:
Case 5: Catamenial hemopneumothorax. Axial T1WI shows a small hyperintense...
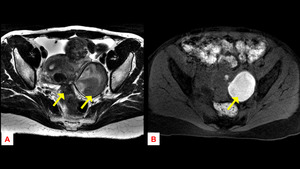
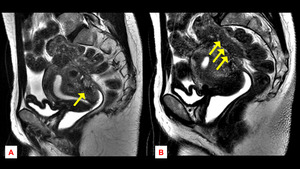
. There also is a left ovarian endometrioma with high signal intensity on T1WI (B) and relatively low signal intensity on T2 image (A).")
Fig. 18:
Case 5: Catamenial hemopneumothorax. Axial T2 image shows a irregular...
 and a retrocervical spiculated margins lesion (B). There also is deep endometriosis infiltrating sigmoid colon/ rectum.")
Fig. 19:
Case 5: Catamenial hemopneumothorax. Sagittal T2 images show a retroverted...