CYSTIC NEOPLASM
1.
Serous cystic neoplasm
Case: Female patient (83 y.o.) asymptomatic (Fig. 1).
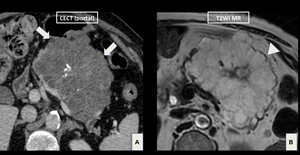
Fig. 1: Note the central calcification and the typical morphological aspect of serous cystic neoplasm with well-circumscribed margins (arrows) and no aggressive features (ductal obstruction or vascular encasement). Multiple small coalescent cysts (honeycomb-like pattern) with radial distribution are also seen (arrowhead).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Serous cystadenomas (SCA) are a benign condition in women (75% x 25%,
F:M)
- Age: 6th-7th decades.
- They are often diagnosed incidentally.
- Slight predominance in the pancreatic head.
- Composed of numerous small cysts (< 1 cm),
which are conjoined in a honeycomb-like pattern.
Tips ⇒ fibrous portion may enhance after contrast injection (central scar) and central calcified areas may appear (stellate pattern).
- CT:the appearance depends on the number of fibrous septa and their degree of enhancement (less fibrous septa = fluid-like attenuation; large number of microcysts = solid appearance on postcontrast phase).
- MR:a SCA appears as a cluster of small cysts within the pancreas,
with no visible communication between pancreatic ducts and the lesion.
- Less common forms: oligocystic (< 6 cysts) (Fig. 2) and solid variants.
- DDX:oligocystic variant ⇒ side-branch IPMNs or pseudocysts.
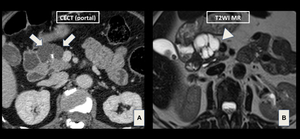
Fig. 2: Note few cysts (arrows) with radial septa converging for a central scar (arrowhead).
References: Grupo DASA, São Paulo/Brazil
Management:
- Referral to a surgeon ⇒symptomatic,
large (> 4 cm),
rapidly growth.
Associations:
- Von Hippel-Lindau (VHL) disease.
2.
Mucinous cystic neoplasm
Case: Female patient (52 y.o.) w/ upper abdominal pain (Fig. 3).
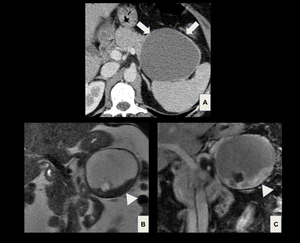
Fig. 3: Axial portal phase CT (A), coronal T2WI (B) and coronal portal phase T1WI (C) demonstrate a large cystic mass arising from the pancreatic tail (arrows). The presence of enhanced mural nodules (arrowheads) suggests a malignant lesion.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Mucinous cystic neoplasms (MCN) are a rare condition of female patients (> 95% of the cases are in women).
- Age:4th-5th decades.
- They range from benign slow-growing cystic adenomas to invasive mucinous cystadenocarcinomas.
- Common locations: body or tail.
- MCN has no communication with the pancreatic ductal system.
- Presence of surrounding ovarian-type stroma (DDX w/ IPMN).
- CT and MR:septated cystic lesion w/ fluid density and postcontrast phase shows enhancement of the cyst wall (+ peripheral calcifications).
- Mural nodules or septal thickening calcification ⇒ presumably a malignant lesion.
Management:
3.
Intraductal papillary mucinous neoplasm (IPMN)
Case: Male patient (60 y.o.) w/ recurrent pancreatitis (Fig. 4).
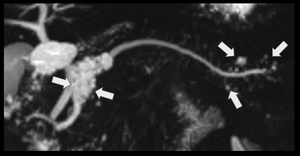
Fig. 4: Coronal MRCP with MIP reconstruction demonstrates side branch IPMNs (arrows) and their direct connection with the adjacent normal sized main pancreatic duct.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- IPMNs are a mucin-producing tumor ⇒ mucinous transformation of the pancreatic ductal epithelium.
- More frequent in men (6th-7th decades).
- Range from noninvasive neoplasm to invasive adenocarcinoma.
- Types:main pancreatic duct (MPD) (Fig. 5),
branch duct (BD),
or a combination of both.
- Relation with pancreatic duct.
- MPD: high malignant transformation. DX: diffuse or segmental ductal dilatation (> 5mm without other causes of obstruction); DDX: chronic pancreatitis (atrophy,
loss of lobulated contour and loss of inherent T1 hyperintensity).
- BD: low malignant transformation; DX: pleomorphic lesion w/.
Pancreatic cysts of > 5 mm in diameter that communicate with MPD; DDX: pseudocysts and serous oligocystic neoplasm.
- "Worrisome features" and "high-risk stigmata" in Table 1 (
 Tanaka et al,
2017).
Tanaka et al,
2017).
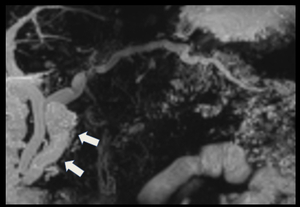
Fig. 5: Coronal MRCP with MIP reconstruction demonstrates diffuse dilatation of the main pancreatic duct, mainly on the pancreatic head (arrows).
References: Grupo DASA, São Paulo/Brazil
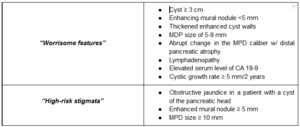
Table 1: "Worrisome features" and "high-risk stigmata"
References: Grupo DASA, São Paulo/Brazil
Management:
- Algorithm for the management is well described in reference #5.
SOLID NEOPLASM
4.
Solid pseudopapillary tumor
Case: Female patient (24 y.o.) w/ abdominal pain (Fig. 6).
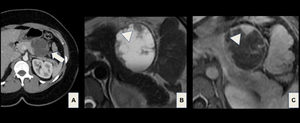
Fig. 6: Axial postcontrast CT (A), axial T2W MR (B) and axial postcontrast T1W (C) MR images show a large, well-defined, heterogeneous mass (arrow) arising from the body and tail of the pancreas. A solid-cystic pancreatic mass (arrowhead) in young woman suggests a Frantz tumor.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Solid pseudopapillary tumor (Frantz tumor) accounts for 1-2% of all pancreatic tumors.
- Prevalence: young adult females (9:1).
- Low malignant potential w/ good prognosis after surgical resection.
Metastases are uncommon.
- Frequently a large,
well-circumscribed mass in the pancreatic tail (followed closely by pancreatic head).
- Hallmark: internal hemorrhage and cystic degeneration.
- MR: hemorrhage usually appears hyperintense on T1WI and has a variable signal on T2WI.
Peripheral calcifications and fluid-fluid or fluid-debris level also can be seen.
- DDX:neuroendocrine tumor (NET).
Management:
5.
Neuroendocrine tumor
Case: Female patient (35 y.o.) w/ hypoglycemia and palpitations (Fig. 7).
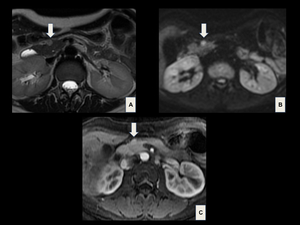
Fig. 7: Insulinoma. MR images demonstrate a small rounded nodule in the pancreas head, characterized by a high signal on (A) T2WI, diffusion restriction on (B) DWI and avid enhancement (C) on postcontrast T2WI (arrows).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- NETs account for 1-5% of pancreatic tumors.
- Prevalence: 5th decade (equal gender distribution).
- Classification: functioning and nonfunctioning tumors.
- Functioning: symptoms related to excessive hormone production (Table 2).
Tend to be multiple and to manifest early (small size).
- Nonfunctioning: late clinical manifestation (large size).
- Tumor size ⇒ risk of malignancy (especially in tumors > 5 cm).
- Malignancy signs: local spread,
vascular invasion,
lymph node involvement,
and organ metastasis.
- Tips ⇒small lesions: well-defined,
hypervascular mass; large lesions:heterogeneous (+/- cystic-necrotic degeneration,
calcification).
- Hallmarks: avid enhancement on the arterial phase and diffusion restriction (Fig. 8).
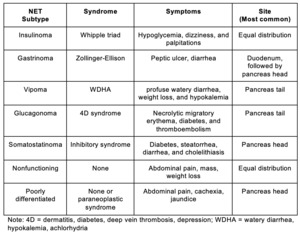
Table 2: NET subtypes characteristics
References: Grupo DASA, São Paulo/Brazil
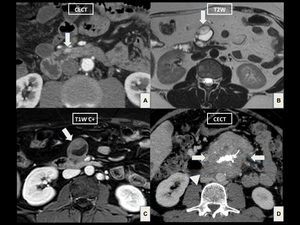
Fig. 8: Three different cases of NET. (A) Gastrinoma: small rounded, hypervascular nodule in the duodenal wall (arrow) at CECT. (B,C) Insulinoma: well-defined, solid-cystic mass in the pancreas head (arrows). (D) Undifferentiated NET: heterogeneous pancreatic mass with central calcifications, extending to peripancreatic structures (arrowhead).
References: Grupo DASA, São Paulo/Brazil
Management:
- Curative therapy: surgical resection.
Associations:
- Multiple endocrine neoplasm type 1,
VHL,
neurofibromatosis type 1,
and tuberous sclerosis.
6.
Neural crest tumors
Case: Female patient (60 y.o.) w/ nausea (Fig. 9).
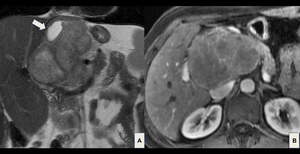
Fig. 9: Coronal T2W (A) and axial arterial phase T1W (B) MR images show a well-circumscribed, heterogeneous pancreatic mass, with a cystic component (arrow) that proved be a schwannoma after surgery. Remember that size and image features may be variables, knowing that the larger lesions are more likely to malignancy.
Teaching points:
- Neural crest (NC) cells ⇒ remarkable capacity of invasiveness,
proliferation,
and pluripotency.
- Pancreatic involvement is uncommon (e.g.
schwannoma and ganglioneuroma).
- Size and image feature variables ⇒ large lesions are associated w/ malignancy.
7.
Metastatic lesions
Case: Female patient (75 y.o.) w/ abdominal pain.
Radical nephrectomy due to renal malignancy 15 years ago (Fig. 10).

Fig. 10: MR images show a solid, well-defined lesion with a heterogeneous signal on T2WI (A), diffusion restriction (B) and hyperenhancement on arterial phase T1WI (C) located in the pancreatic tail (arrows). (D) Another hypervascular mass is detected in pancreatic head (arrowhead).
References: Grupo DASA, São Paulo/Brazil
Teaching point:
- Pancreatic metastases account for 2-5% of pancreatic malignancies.
- Common primaries:renal cell carcinoma (RCC) and lung carcinoma,
followed by breast carcinoma,
colorectal carcinoma,
and melanoma.
- RCC metastasis may manifest belatedly (e.g.
6-12 years after nephrectomy).
- Imaging features: focal,
multifocal or diffuse; solid (more common) or cystic,
and the enhancement may be similar to the primary neoplasm.
8.
Lymphoproliferative tumors
Case: Male patient (54 y.o.) w/ AIDS (Fig. 11).
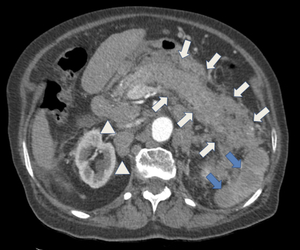
Fig. 11: CECT image on arterial phase demonstrates a diffusely enlarged pancreas associated with ill-defined, infiltrative peripancreatic tissue (arrows). Multiple enlarged lymph nodes (arrowheads) and splenic nodules (blue arrows) are also seen.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- The most common lymphoproliferative pancreatic disease (LPD) is the non-Hodgkin lymphoma B-cell subtype.
- Two forms:primary and secondary.
- Primary:rare; secondary: direct extension from peripancreatic lymphadenopathy.
- Tip: consider LPD in immunocompromised patients.
- Imaging findings: focal or diffuse appearance.
- Focal ⇒pancreas head.
- Diffuse (infiltrative) ⇒enlargement of all pancreas (simulate acute pancreatitis) (Fig. 12).
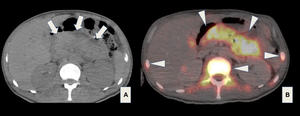
Fig. 12: Axial unenhanced CT (A) and axial PET-CT with FDG (B) images show a diffuse enlargement of the entire pancreas (arrows) associated with FDG uptake on the pancreas and skeleton (arrowheads). The diagnosis was consistent with lymphoma.
INFLAMMATION-RELATED LESIONS
9.
Pseudocyst
Case: Female patient (40 y.o.) w/ previous pancreatitis (Fig. 13).
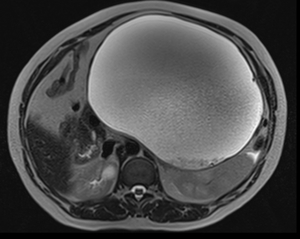
Fig. 13: Axial T2W MR image shows a very large, well-defined cystic mass in retroperitoneum consistent with pseudocyst.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Pseudocysts are the most common cystic lesions of the pancreas.
- They appear 4 weeks after interstitial edematous pancreatitis (IEP) episode.
- Imaging findings: a well-circumscribed cystic mass with no solid components.
At MR,
pseudocysts are uniformly hyperintense on T2WI (only fluid with no nonliquefied components).
- Tip: peripancreatic in location (intrapancreatic is also seen).
Management:
- Drainage if infected or symptomatic.
10.
Walled-off necrosis
Case: Male patient (44 y.o.).
Previous necrotizing pancreatitis (Fig. 14).
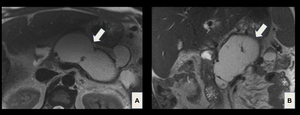
Fig. 14: Axial (A) and coronal (B) T2W MR images demonstrate a well-defined lobulated fluid collection with thickened wall consistent with walled-off necrosis (arrows).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Walled-off necrosis (WON) arises from the organization of acute necrotic collection 4 weeks after a necrotizing pancreatitis episode.
- WON contains necrotic fat and/or pancreatic tissue (nonliquefied debris within the fluid).
- The most common location of occurrence is in the peripancreatic space but can appear in pancreatic parenchyma,
or in both sites (coalescent collection).
Management:
- Often requires either a large bore catheter for drainage or necrosectomy.
11.
Groove pancreatitis
Case: Male patient (50 y.o.) w/ abdominal pain (Fig. 15).
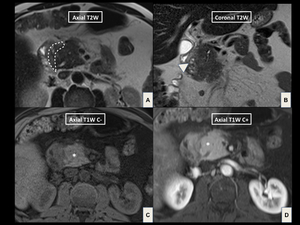
Fig. 15: (A,B) T2W MR images demonstrate an infiltrative “sheetlike" soft tissue in the pancreaticoduodenal groove (dashed contour) associated with small cysts in the duodenal wall (arrowhead). (C,D) On T1WI, note the thickening duodenal wall and the maintenance of normal glandular signal of the pancreas head (*).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Groove pancreatitis (pancreaticoduodenal pancreatitis) is a type of pancreatitis that affects the "groove" between the pancreatic head,
duodenum,
and common bile duct.
- Forms: pure and segmental.
- Pure form: ill-defined,
inflammatory changes in the groove (“sheetlike” curvilinear crescentic shape).
- Segmental form: pancreaticoduodenal groove involvement can be obscured by masslike enlargement of pancreatic head.
12.
Pseudotumor of chronic pancreatitis
Case: Female patient (60 y.o.) w/ chronic pancreatitis and abdominal pain (Fig. 16).
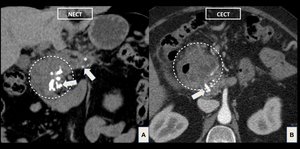
Fig. 16: (A,B) CT images demonstrate a heterogeneous, ill-defined mass in the pancreatic head associated with adjacent soft tissue obliterating the pancreaticoduodenal groove (circle). Note multiple calcifications in head and body of the pancreas (arrows), and the diffusely enlarged MPD (*), findings related to chronic pancreatitis.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Chronic pancreatitis is a risk factor for pancreatic cancer.
However,
a pancreatic mass may also occur secondary an inflammation lesion (pseudotumor).
- The differentiation between pseudotumor and pancreatic cancer may be challenging.
- CT,
MR,
and EUS are widely used in clinical practice.
PET tends to be more sensitive than CT in detecting lesions less than 2 cm.
SYSTEMIC DISEASES
13.
IgG4-related disease
Case: Male patient (74 y.o.) w/ impairment of renal function (Fig. 17).
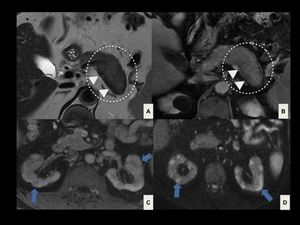
Fig. 17: IgG4-related disease with autoimmune pancreatitis and renal involvement. Axial T2W (A) and postcontrast T1W (B) MR images show diffuse enlargement of the pancreas, with the absence of pancreatic clefts and a sharp outline ("sausagelike appearance”) (dashed circles), and a hypointense halo of fibrosis (arrowheads). Axial postcontrast T1W (C) and DWI (D) MR images demonstrate multiple wedge-shaped lesions in both kidneys (blue arrows).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Autoimmune pancreatitis (AIP) is the most common presentation of IgG4-related disease and is a specific form of chronic pancreatitis.
- Types:type 1 (lymphoplasmacytic sclerosing pancreatitis) and type 2 (idiopathic duct-centric chronic pancreatitis).
- Distinct features: type 1 is the pancreatic manifestation of IgG4-related disease,
while type 2 has a different histologic and clinical profile (no elevation of serum IgG4 concentration or presence of autoantibodies).
- Diffuse or focal enlargement of the pancreas and irregular narrowing of the MPD + loss of lobulations w/ a surrounding capsule-like rim ="sausagelike" appearance.
- Capsule-like rim ⇒specific finding of AIP (demonstrated at MR and CT).
- DDX: carcinoma (focal form) and acute pancreatitis (diffuse form).
Associations:
- Cholangitis,
inflammatory pseudotumors,
IgG4-related hepatopathy,
membranous nephropathy,
chronic sclerosing pyelitis,
prostatitis,
retroperitoneal fibrosis.
14.
Erdheim-Chester
Case: Female patient (45 y.o.) w/ nausea and abdominal pain (Fig. 18).
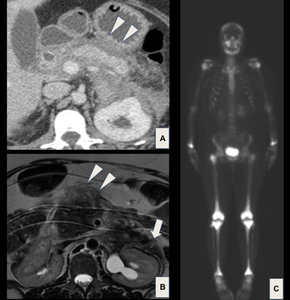
Fig. 18: Axial postcontrast CT (A), axial T2WI MR (B) and frontal bone scan (C). Note a heterogeneous soft tissue in the retroperitoneum encasing the kidneys (arrow) and pancreas (arrowheads). These findings plus the uptake in the metaphyseal regions of the femur and distal radius are characteristic features of Erdheim-Chester disease.
Teaching points:
- A rare form of non-Langerhans cell histiocytosis characterized by the accumulation of clear foamy histiocytes.
- Broad clinical manifestations.
Bone is the most common site affected.
- 2/3 of patients demonstrate retroperitoneal involvement.
NON-ADENOCARCINOMA PANCREATIC LESIONS: MIMICKING LESIONS
15.
Annular pancreas
Case: Male patient (16 y.o.) asymptomatic (Fig. 19).
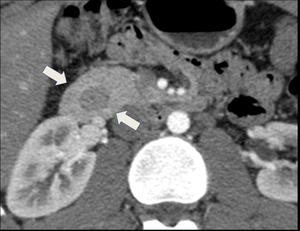
Fig. 19: Axial postcontrast CT demonstrates pancreatic tissue completely encircling the duodenum (arrows).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Second most common pancreatic congenital anomaly.
- AP is characterized by pancreatic tissue partially or completely encircling the second part of the duodenum (may cause gastrointestinal obstruction).
16. Bifid tail of the pancreas
Case: Male patient (55 y.o.) asymptomatic (Fig. 20).
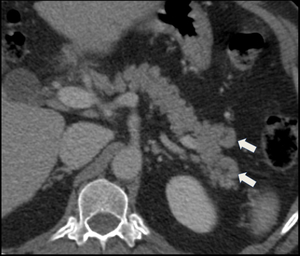
Fig. 20: Axial postcontrast CT shows a rare anomaly, also known as bifid pancreas or fishtail pancreas (arrows).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Rare developmental anatomic branching anomaly (“fishtail pancreas”).
- Commonly it is an incidental finding.
17.
Ectopic pancreas
Case: Male patient (43 y.o.) asymptomatic (Fig. 21).
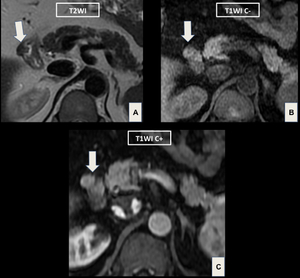
Fig. 21: MR images demonstrate a small solid tissue in the duodenal wall with signal intensity similar to pancreatic parenchyma (arrows), findings that should be considered as an ectopic pancreas.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- The ectopic pancreas can be found in the stomach (more commonly),
duodenum,
jejunum,
Meckel diverticulum,
or ileum.
- Ectopic tissue usually measures 0.5 - 2.0 cm.
- Complications: stenosis,
ulceration,
inflammation,
bleeding,
and intussusception.
18.
Intrapancreatic accessory spleen
Case: Male patient (22 y.o.) asymptomatic (Fig. 22).
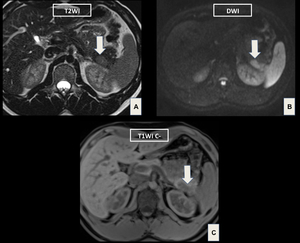
Fig. 22: MR images show a well-circumscribed nodule in the pancreatic tail. Note the same nodule signal intensity when compared to spleen. These findings are typically seen on the intrapancreatic accessory spleen.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Commonly seen in the pancreatic tail.
- Hallmark: maintenance of the same attenuation/signal of the spleen.
- Tip: small,
well-defined ovoid mass in pancreatic tail.
- DDX: NET (differentiation with technetium 99m [99mTc] sulfur colloid scintigraphy and 99mTc heat-damaged red blood cell scintigraphy).
19.
Fatty infiltration-replacement
Case: Female patient (15 y.o.) asymptomatic (Fig. 23).
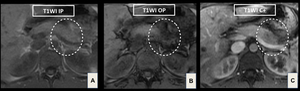
Fig. 23: T1W IP (A), T1W OP (B) and portal venous phase T1W (C) MR images demonstrate a focal lesion in the pancreatic body/tail (dashed circle). This area shows a marked decrease in signal intensity on T1WI OP compared with T1WI IP. The hypoenhancement pattern of the lesion is also seen.
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Fatty infiltration-replacement can be focal (rare) or diffuse.
- Diffuse form: elderly or obese patients (also seen in chronic pancreatitis and cystic fibrosis) (Fig. 24).
- Focal form may simulate a tumor.
A spared area within diffusely fatty replaced pancreas also simulates a lesion.
- Geographic predilection for the anterior aspect of the pancreatic head.
Posterior aspect is usually spared.
- CT and MR demonstrate attenuation/signal of macroscopic fat,
the absence of mass effect,
and nondeformity of pancreas configuration.
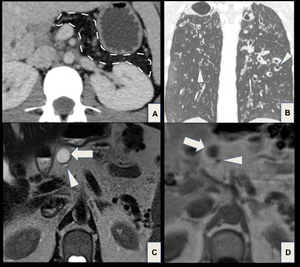
Fig. 24: Two different cases of diffuse pancreatic fatty replacement. (A,B) Cystic fibrosis. Portal venous phase CT scan shows complete fatty replacement of the pancreas (dashed contour) (A). Chest CT scan demonstrates saccular bronchiectasis (arrowheads) in both lungs (B). (C,D) Elderly patient. T2W (C) and T1W (D) MR images demonstrate a cystic lesion (arrows) in pancreas with fatty infiltration-replacement. Note a thin MPD through the pancreatic head (D).
References: Grupo DASA, São Paulo/Brazil
20.
Radiation-related findings
Case: Male patient (55 y.o.) w/ unresectable pancreatic adenocarcinoma (Fig. 25).
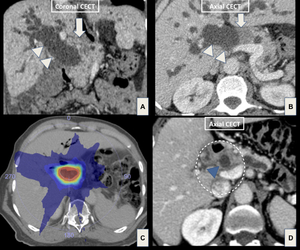
Fig. 25: (A,B) Pretreatment CT imaging assessment on portal phase shows an ill-defined, hypoattenuating mass in the head of the pancreas (arrows) with biliary tree dilatation (arrowheads). (C) Axial CT obtained for SBRT planning with a dose of 35 Gy and daily IGRT (five fractions of 700 cGy). (D) Posttreatment evaluation two years after RT, note decreasing of the pancreatic lesion (dashed circle) and biliary tree dilatation (blue arrowhead). The differentiation between viable tumor and radiation-induced changes is hard and usually not possible. PET-CT imaging assessment can help to distinguish it.
References: Grupo DASA, São Paulo/Brazil
Teaching points
- The pancreas is an organ relatively radioresistant.
Early radiation-induced effects are uncommon.
- Typical late effects are pancreatic atrophy and calcifications,
mimicking the finding of chronic pancreatitis.
- Sometimes,
a radiation-induced effect may present mass-like appearance.
- Follow-up aids in differentiation between posttreatment alterations and tumor.
21.
Postoperative-related findings
Case: Patient female (25 y.o.) after distal pancreatectomy (Fig. 26).
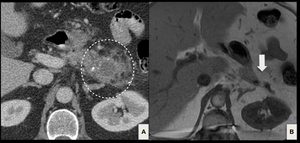
Fig. 26: Acute pancreatitis in a postoperative patient after distal pancreatectomy performed for a pancreatic tail Frantz tumor. (A) Portal venous CT through the surgical bed in early postsurgical period shows peripancreatic fluid and fat stranding (dashed circle). Follow-up T1W MR image obtained 1 year later demonstrates normal postoperative findings (arrow).
References: Grupo DASA, São Paulo/Brazil
Teaching points:
- Some pancreatic imaging findings may be misinterpreted after pancreatic surgery.
- Pitfalls: edema (gastrojejunostomy or duodenojejunostomy); perivascular cuffing (surgical bed and surrounding the celiac axis,
and superior mesenteric and hepatic arteries).
- Follow-up examinations usually demonstrate regression of postoperative findings.

 and no aggressive features (ductal obstruction or vascular encasement). Multiple small coalescent cysts (honeycomb-like pattern) with radial distribution are also seen (arrowhead). References: Grupo DASA, São Paulo/Brazil")
 with radial septa converging for a central scar (arrowhead). References: Grupo DASA, São Paulo/Brazil")
, coronal T2WI (B) and coronal portal phase T1WI (C) demonstrate a large cystic mass arising from the pancreatic tail (arrows). The presence of enhanced mural nodules (arrowheads) suggests a malignant lesion. References: Grupo DASA, São Paulo/Brazil")
 and their direct connection with the adjacent normal sized main pancreatic duct. References: Grupo DASA, São Paulo/Brazil")
. References: Grupo DASA, São Paulo/Brazil")

, axial T2W MR (B) and axial postcontrast T1W (C) MR images show a large, well-defined, heterogeneous mass (arrow) arising from the body and tail of the pancreas. A solid-cystic pancreatic mass (arrowhead) in young woman suggests a Frantz tumor.
References: Grupo DASA, São Paulo/Brazil")

 T2WI, diffusion restriction on (B) DWI and avid enhancement (C) on postcontrast T2WI (arrows). References: Grupo DASA, São Paulo/Brazil")
 Gastrinoma: small rounded, hypervascular nodule in the duodenal wall (arrow) at CECT. (B,C) Insulinoma: well-defined, solid-cystic mass in the pancreas head (arrows). (D) Undifferentiated NET: heterogeneous pancreatic mass with central calcifications, extending to peripancreatic structures (arrowhead). References: Grupo DASA, São Paulo/Brazil")
 and axial arterial phase T1W (B) MR images show a well-circumscribed, heterogeneous pancreatic mass, with a cystic component (arrow) that proved be a schwannoma after surgery. Remember that size and image features may be variables, knowing that the larger lesions are more likely to malignancy.")
, diffusion restriction (B) and hyperenhancement on arterial phase T1WI (C) located in the pancreatic tail (arrows). (D) Another hypervascular mass is detected in pancreatic head (arrowhead). References: Grupo DASA, São Paulo/Brazil")
. Multiple enlarged lymph nodes (arrowheads) and splenic nodules (blue arrows) are also seen. References: Grupo DASA, São Paulo/Brazil")
 and axial PET-CT with FDG (B) images show a diffuse enlargement of the entire pancreas (arrows) associated with FDG uptake on the pancreas and skeleton (arrowheads). The diagnosis was consistent with lymphoma.")

 and coronal (B) T2W MR images demonstrate a well-defined lobulated fluid collection with thickened wall consistent with walled-off necrosis (arrows). References: Grupo DASA, São Paulo/Brazil")
 T2W MR images demonstrate an infiltrative “sheetlike" soft tissue in the pancreaticoduodenal groove (dashed contour) associated with small cysts in the duodenal wall (arrowhead). (C,D) On T1WI, note the thickening duodenal wall and the maintenance of normal glandular signal of the pancreas head (*). References: Grupo DASA, São Paulo/Brazil")
 CT images demonstrate a heterogeneous, ill-defined mass in the pancreatic head associated with adjacent soft tissue obliterating the pancreaticoduodenal groove (circle). Note multiple calcifications in head and body of the pancreas (arrows), and the diffusely enlarged MPD (*), findings related to chronic pancreatitis. References: Grupo DASA, São Paulo/Brazil")
 and postcontrast T1W (B) MR images show diffuse enlargement of the pancreas, with the absence of pancreatic clefts and a sharp outline ("sausagelike appearance”) (dashed circles), and a hypointense halo of fibrosis (arrowheads). Axial postcontrast T1W (C) and DWI (D) MR images demonstrate multiple wedge-shaped lesions in both kidneys (blue arrows). References: Grupo DASA, São Paulo/Brazil")
, axial T2WI MR (B) and frontal bone scan (C). Note a heterogeneous soft tissue in the retroperitoneum encasing the kidneys (arrow) and pancreas (arrowheads). These findings plus the uptake in the metaphyseal regions of the femur and distal radius are characteristic features of Erdheim-Chester disease.")
. References: Grupo DASA, São Paulo/Brazil")
. References: Grupo DASA, São Paulo/Brazil")
, findings that should be considered as an ectopic pancreas. References: Grupo DASA, São Paulo/Brazil")

, T1W OP (B) and portal venous phase T1W (C) MR images demonstrate a focal lesion in the pancreatic body/tail (dashed circle). This area shows a marked decrease in signal intensity on T1WI OP compared with T1WI IP. The hypoenhancement pattern of the lesion is also seen. References: Grupo DASA, São Paulo/Brazil")
 Cystic fibrosis. Portal venous phase CT scan shows complete fatty replacement of the pancreas (dashed contour) (A). Chest CT scan demonstrates saccular bronchiectasis (arrowheads) in both lungs (B). (C,D) Elderly patient. T2W (C) and T1W (D) MR images demonstrate a cystic lesion (arrows) in pancreas with fatty infiltration-replacement. Note a thin MPD through the pancreatic head (D). References: Grupo DASA, São Paulo/Brazil")
 Pretreatment CT imaging assessment on portal phase shows an ill-defined, hypoattenuating mass in the head of the pancreas (arrows) with biliary tree dilatation (arrowheads). (C) Axial CT obtained for SBRT planning with a dose of 35 Gy and daily IGRT (five fractions of 700 cGy). (D) Posttreatment evaluation two years after RT, note decreasing of the pancreatic lesion (dashed circle) and biliary tree dilatation (blue arrowhead). The differentiation between viable tumor and radiation-induced changes is hard and usually not possible. PET-CT imaging assessment can help to distinguish it. References: Grupo DASA, São Paulo/Brazil")
 Portal venous CT through the surgical bed in early postsurgical period shows peripancreatic fluid and fat stranding (dashed circle). Follow-up T1W MR image obtained 1 year later demonstrates normal postoperative findings (arrow). References: Grupo DASA, São Paulo/Brazil")