ECR 2019 / C-3026

Radiologic Approach to Erectile Dysfunction. Main causes, diagnosis and therapeutic options in interventional radiology.
Congress:
ECR 2019
Poster Number:
C-3026
Type:
Educational Exhibit
Keywords:
Haemodynamics / Flow dynamics, Education and training, Arteriosclerosis, Venous access, Embolisation, Education, Ultrasound-Power Doppler, Ultrasound-Colour Doppler, Catheter venography, Vascular, Interventional vascular, Genital / Reproductive system male
Authors:
J. Periáñez1, E. Crespo1, A. Villalba Gutiérrez2, A. Hermosin Pena1, G. Monedero Herrador1, E. E. Daguer Tamayo1; 1Madrid/ES, 2Leganés/ES
DOI:
10.26044/ecr2019/C-3026

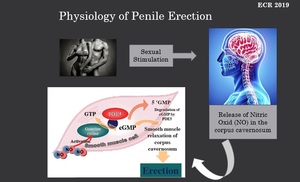
Fig. 1:
Physiology of Penile Erection.
NO: Nitric Oxide.
GTP:guanosine...

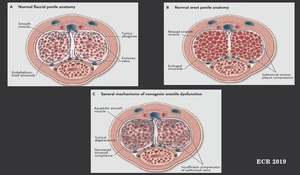
Fig. 2:
Veno-oclusive mechanism in penile erection.
A- Normal flacid penis. Smooth...

Fig. 3:
Main Causes of Erectile Dysfunction.

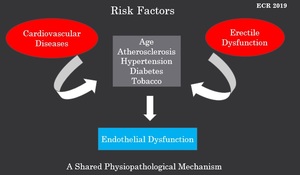
Fig. 4:
Risk Factors in Erectile Dysfunction. Endothelial Dysfunction as a shared...
. Eur Urol ; 44: 352-354.")
Fig. 5:
The Hypothesis of Arterial Diameter.
- Given coronary arteries diameter,...