ECR 2019 / C-3040

Pancreas in children: from head to tail
Congress:
ECR 2019
Poster Number:
C-3040
Type:
Educational Exhibit
Keywords:
Paediatric, Pancreas, Abdomen, MR, Ultrasound, CT, Education, Education and training
Authors:
M. Gonzalo Carballés1, A. Coma2, X. Merino Casabiel1, L. Riaza Martin3, L. Riera1, A. Castellote1, J. Piqueras1, J. C. Carreño1, E. Vazquez1; 1Barcelona/ES, 2Lleida/ES, 3Esplugues de Llobregat/ES
DOI:
10.26044/ecr2019/C-3040

Fig. 1:
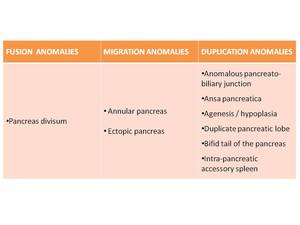
Pancreas develops from two anlagens that arise from the endodermal lining of...
, migration (annular pancreas, ectopic pancreas) or a duplication anomalies (number or morphology variation).")
Fig. 2:
Anatomic anomalies of the pancreas are classified as either fusion (pancreas...
 over the pancreatic duct (red arrow) which is draining separately at the minor papilla. The ventral duct is not visualized suggesting type-II pancreas divisum.")
Fig. 3:
Pancreas divisum in a 5-year-old boy who presented with acute pancreatitis. ...
. MRI images depict atrophy (yellow arrow)of the pancreas associated with an irregular dilated main pancreatic duct, which is draining separately into the minor papilla, signs related to recurrent pancreatitis.")
Fig. 4:
Pancreas divisum in a 16-year-old boy with recurrent pancreatitis. Contrast...
 draining with the ventral pancreatic duct (red star) through the major papilla and a dilated dorsal pancreatic duct (yellow star) draining separately in to the minor papilla suggestive of a classic pancreatic divisum.")
Fig. 5:
MRCP images demonstrated a dilated external biliary duct (green star) draining...
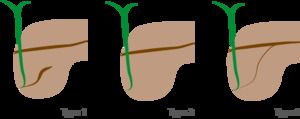
: absent fusion between de ventral duct of Wirsung and the dorsal duct of Santorini
Type-II (Absent ventral duct): minor papilla drains all the pancreas
Type -III (functional): rudimentary connection between dorsal and ventral ducts")
Fig. 6:
Type-I (classic): absent fusion between de ventral duct of Wirsung and the...
 that completely encircles the second portion of the duodenum (green star).")
Fig. 7:
Annular pancreas in a 22-year-old patient. Fat-saturated T1 weighted MRI shows...
.")
Fig. 8:
A 4 year-old boy with repeated episodes of vomiting and epigastric distention ...
. Duodenojejunal junction was correctly located. Duodenoduodenostomy was performed, with no complications (c).")
Fig. 9:
The 4-year-old patient presented above underwent abdominal surgery that...

Fig. 10:
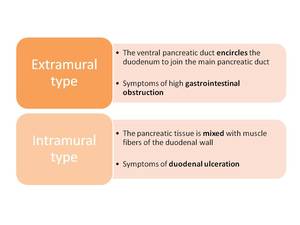
Types of annular pancreas

Fig. 11:
Heterotopic pancreas in a 19-month-old girl with hematemesis. MRI: Depicts a...
.")
Fig. 12:
MR cholangiography demonstrates the abnormally long common channel of the...
 with recurrent pancreatitis. T2WI-MR show dilated proximal intrahepatic bile ducts (red arrow), dilated extrahepatic bile duct (common bile duct and proximal choledoc, green arrow), dilated cystic duct (yellow arrow) and a mild dilatation of the main pancreatic duct (blue arrow), which is compressed by the choledocal cyst. It was not possible to identify the anomalous pancreaticobiliary junction, but it was confirmed by surgery.")
Fig. 13:
A 18-month-old child with congenital choledochal cyst (type Ic of Todani...
 and a congenital variant of the ductal pancreatic system known as “ansa pancreatica” with a dominant Santorini accessory duct (green circle).")
Fig. 14:
T2WI MRI images of an adult patient show a normal-sized pancreatic gland with...
 forming an unusual reversed S-shaped curve (yellow arrow), communicating the ventral (red arrow) and dorsal ducts at the pancreatic head, that drains into the minor papilla. These findings support the diagnose of ansa pancreatica.")
Fig. 15:
3D-MRCP image reveals a dominant Santorini accessory duct (green arrow) forming...

Fig. 16:
Patient with congenital pancreatic hypoplasia due to HNF1-ß gene mutation.
 connected with the main pancreatic gland and containing an aberrant duct (green arrow).")
Fig. 17:
Young patient with an accessory pancreatic lobe (yellow arrow) connected with...
 misdiagnosed as a pancreatic tumour. T2WI: hyperintense to pancreas T1WI+Gd: slightly hypoenhancing compared to pancreas, DWI/ADC: restricted diffusion. Technetium-99m SPECT was performed and showed an increased focal uptake within pancreatic tail compatible with focal splenosis.")
Fig. 18:
A 16 year-old girl with hereditary spherocytosis, who had undergone...
 is believed to be the only imaging modality that can identify the lesions.")
Fig. 19:
A 2-month-old patient with persistent hypoglycemia. 18F-DOPA PET-CT...
")
Fig. 20:
Diffuse fatty replacement and pancreatic atrophy in a 14-year-old girl with...
 in the uncinate process, head, body and tail of the pancreas. MR images confirmed a nearly complete replacement of pancreas by several macroscopic cysts, without signs of complication.")
Fig. 21:
Pancreatic cystosis in a 12-year-old boy with Cystic Fibrosis. Transverse...
 and a hypervascular nodule in the pancreatic head compatible with a neuroendocrine tumor (red arrow).")
Fig. 22:
A 19 year-old boy with Von Hippel Lindau Syndrome diagnosed at the age of 7. A...
. Doppler showed no vascularity (b). Linear transducer US depicts a thin echogenic wall (c). Abdominal MR imaging discloses a lesion related to the pancreatic tail in the left upper abdomen with homogeneous hypointensity on T1WI (yellow arrow), (d) and slightly heterogeneous hyperintensity on fat-sat T2WI (yellow arrow)(e). Low-dose unenhanced abdominal CT scanning used to guide fine-needle aspiration sampling reveals a rounded, well-defined, homogenic, slightly hypodense lesion at the pancreatic tail. There were no calcifications (f).")
Fig. 23:
Intrapancreatic duplication cyst in a 10-year-old girl with repeated episodes...
 (yellow arrow) was demonstrated, adjacent to pancreatic tail (yellow star). Note the fluid-fluid level within the mass (green star). Abdominal MR imaging reveals a large left-side cyst opening the pancreatic tail with a slighty hyperintensity on T1WI and predominantly hyperintense on T2WI with fluid-fluid levels (blood or debris). No restriction diffusion was depicted.")
Fig. 24:
Intrapancreatic duplication cyst in a 5-year-old girl with abdominal...
 MR images obtained 2 months later show on the T2-weighted MRI sequence a walled-off, heterogeneous peripancreatic collection, with a fluid component that appears hyperintense and necrotic non liquefied material that appears hypointense, that arises from the tail of the pancreas and extends to the mesocolon (green arrow). An absence of restriction on diffusion sequences is depicted (green star). The findings were compatible with necrotic fat tissue (walled-off necrosis).")
Fig. 25:
Late complication of an acute pancreatitis in a 12-year-old girl who underwent...

Fig. 26:
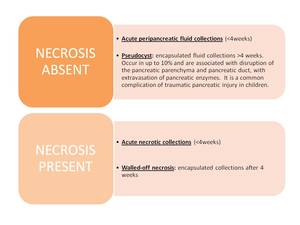
Pancreatic fluid collections are defined by presence or absence of necrosis
, atrophy of the pancreatic gland, punctuate calcification throughout the pancreatic parenchyma (green arrow) and a 6mm calculi within the proximal segment of the main pancreatic duct (red star). T2WI thick slab MRCP image shows irregularly dilated main pancreatic duct and side branches, giving chain-of-lakes appearance. Notice the pancreatic duct stone.")
Fig. 27:
Hereditary chronic pancreatitis in a 7-year-old-boy with recurrent episodes of...
 with an irregular mild-dilated main pancreatic duct and side branches (green arrow). T2WI thick slab MRCP image shows irregularly dilated main pancreatic duct and side branches. Note the 5mm calculi within the proximal segment of the main pancreatic duct on the pancreatic head (red star).")
Fig. 28:
Hereditary chronic pancreatitis in a 13-year-old-girl with recurrent episodes...
 and peripancreatic fluid (green star). Following studies demonstrated an autoimmune etiology. Note the transpyloric feeding tube placement (red star).")
Fig. 29:
Acute edematous pancreatitis in a 2-year-old boy with abdominal pain and fever...
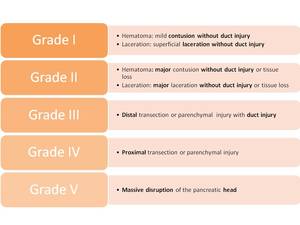
. Advance one grade for multiple injuries up to grade III. Proximal injury: to the right of the superior mesenteric vein.")
Fig. 30:
Pancreatic injury scale (American Association for the Surgery of Trauma)....
 with peripancreatic fat strading (green star). Emergency CT reveals a major contusion of the uncinate process and the pancreatic head (yellow arrow) with peripancreatic and intraperitoneal free fluid (red star). There is no pancreatic duct injury a no active bleeding.")
Fig. 31:
Grade II pancreatic injury in a 10-year-old boy who sustained a blunt abdominal...
. Distal pancreatectomy and esplenectomy were performed (yellow circle). There is a high suspicion of pancreatic ductal injury, corresponding to a grade III pancreatic injury as per the American Association for Surgery in Trauma (AAST).")
Fig. 32:
A 16 year-old boy with a football match blunt abdominal trauma. Emergency...
 with peripancreatic fluid (red star). MR images obtained three weeks later reveal disruption of the pancreatic duct with a large fluid collection (green star) adjacent to pancreatic tail, spleen and stomach . Thick slab MRCP shows communication of the pancreatic duct (red arrow) with a large fluid collection.")
Fig. 33:
Grade III pancreatic injury in a 12-year-old boy who sustained a blunt...

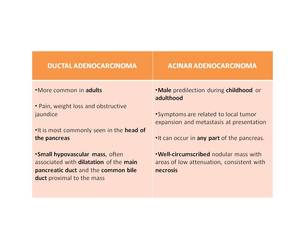
Fig. 34:
Types of adenocarcinoma
. Delayed-phase T1 weighted images obtained after gadolinium administration show poor enhancement of the lesion (green arrow). The lesion presents diffusion restriction on DW images (red star).")
Fig. 35:
Neuroendocrine tumour of the pancreas in a 16-year-old with MEN-1 history....
. Secondary biliary (green arrow) and pancreatic ductal dilatation (red arrow) is seen. Pathology confirmed a pseudopapillary neoplasm of the pancreas.")
Fig. 36:
A 14 year-old girl with epigastric pain and raised amylase, treated as acute...
 and cystic mass (yellow star) that arises from the body of the pancrees. Axial T1-weightened image shows a well-defined heterogeneous mass with areas of high signal compatible with blood products (red arrow). T2-weighted images show a thick fibrous capsule (blue arrow), seen as a discontinuous rim of low signal intensity. Delayed-phase T1 weighted images obtained after gadolinium administration show heterogeneous enhancement of solid portion (green arrow). The solid portion of the lesion presents diffusion restriction on DW images (red star). Note the mass effect on the surrounding structures.")
Fig. 37:
Solid-cystic papillary tumor in a 12-year-old girl who presented with...
 and a heterogenous hypoechoic pelvic mass (green arrow) that contains gas (red star).")
Fig. 38:
A 12-year-old girl who presented to the emergency room with lower-abdominal...
 with patchy areas of nonenhancement (yellow star), soft-tissue pelvic mass with ill-defined margins and gas (red star) involving a small bowel loop (green arrow). Renal involvement is also depicted, note the focal hypodense lesions at the inferior pole of the right kidney without associated hydronephrosis (red arrow). A soft-tissue mass is present within the abdominal wall (green star). Pleural thickening with pleural effusion (blue arrow). The findings were compatible with Burkitt lymphoma with extranodal involvement (pathologically proven).")
Fig. 39:
An enhanced CT was performed to the 12-year-old patient presented above. CT...
, presenting diffusion restriction on DWI/ADC (green arrows). Multiple lung metastases were depicted (green circle).")
Fig. 40:
A 16-year-old boy who underwent abdominal surgery due to an urinary bladder...
, multiple hepatic metastases (red arrow) and necrotic pancreatic lesions within the body and tail (yellow arrow).")
Fig. 41:
Retroperitoneal pleomorphic undifferentiated sarcoma refractory to treatment in...