I- Anatomical sum-up about sinonasal cavities :
Although complicated,
adequate knowledge of paranasal sinuses is essential in order to guide functional endoscopic surgery.
CT is the modality of choice in imaging offering multiplanar reconstruction.
It retains a place for pre-surgical morphological assessment as well as for the analysis of bone structures of the facial bone and skull base.
What is the technique of CT ?
- Patient in supine position and axial images of the sinuses are acquired with 0.625 collimation and from this raw data sagittal and coronal reformations are obtained using both soft tissue and bone window algorithms.
-Thus,
coronal,
sagittal or oblique reformations are helpful for a good interpretation.
- The anatomical study is correctly evaluated without the use use of IV injected ionated contrast material.
Nasal cavity: Fig. 1
It is a median cavity,
connected with the base of the skull (superiorly),
the roof of the mouth (inferiorly) and the orbits (laterally).
The nasal septum divides the nasal cavity into two halves that communicate with the paranasal sinuses via the naso-sinus meatus.
It also communicate behind with the nasopharynx via the posterior nasal apertures (the choanae).
The anterior superior septum is composed of cartilage and the posterior portion is formed by bones,
including the vomer and the perpendicular plate of the ethmoid bone.
The lateral nasal wall is formed of three bulbous projections,
namely the superior,
middle,
and inferior turbinates (conchae),
which divide the nasal cavity into superior,
middle,
and inferior meati.
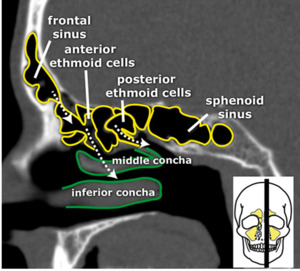
Fig. 2: Sagittal CT image.
The lateral nasal wall.
References: R.L. Widya,LUMC, start Radiology
Paranasal sinuses are the frontal,
ethmoid,
sphenoid and maxillary sinuses,
housed within the bones of the skull.
- The frontal sinuses: Two irregular air-filled cavities situated
between the tables of the frontal bone.
They are seperated from the anterior cerebral fossa via the interior table bone.
Each frontal sinus opens into the corresponding middle meatus through the fronto-nasal duct/recess.
- The maxillary sinuses:
Two air-filled cavities within the body of the maxillae.
Each one communicate with the middle meatus through the maxillary ostium and,
subsequently,
through the infundibulum and semilunar hiatus.
- The ethmoidal cells:
All of them open into the lateral wall of the nasal cavity through their corresponding ostia.
they are divided into three groups : anterior,
middle and posterior.
They are seperated via the ground lamella which is a lateral bony extent of
the middle nasal concha which fuses to the lamina papyracea.
Anterior and middle ethmoidal air cells drain into middle meatus via hiatus semilunaris.
The posterior ethmoidal cells are situated between the ground lamella and the sphenoidal sinus,
draining into the superior meatus and,
subsequently,
into the spheno-ethmoidal recess.
The Agger nasi air cells are the most anterior ethmoidal air cells,
lying anterolateral and inferior to the fronto-ethmoidal recess and anterior and above to the attachement of the middle turbinate.
They drain into the ethmoidal infundibulum and are lateral to the orbit,
the lacrimal sac and the nasolacrimal duct.
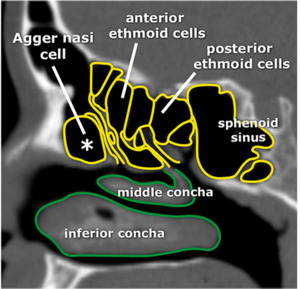
Fig. 3: Sagittal CT image.
Agger nasi cell (*); most anterior ethmoid cell.
References: R.L. Widya,LUMC, start Radiology
The sphenoidal sinuses:
They are the most posterior paranasal sinuses and drain into the superior meatus via the spheno-ethmoidal recess.
A bone septum divide the two sphenoidal sinuses.
They have a contact with:
*The pituitary gland and the optic chiasm at the top.
*Pharyngeal fornix down.
*The cavernous sinus laterally
*Nasal cavity in front.
The uncinate process is a thin,
mucosal lined osseous prominence,
with its superior free edge forming the semilunar hiatus that opens directly into the middle meatus.
Anteriorly,
it originates the postero-medial
edge of the naso-lacrimal duct.
The infundibulum is situated laterally to the uncinate process,
connecting the maxillary and ethmoidal sinuses ostia to the semilunar
hiatus.
The major draining ostia of the paranasal sinuses are:
Draining the frontal,
maxillary sinuses and anterior and middle third of the ethmoid sinuses,
and including the frontal sinus ostium,
frontal recess,
maxillary sinus ostium,
infundibulum,
uncinate process,
ethmoid bulla ethmoidal,
semilunar hiatus,
middle nasal concha and nasal meatus.
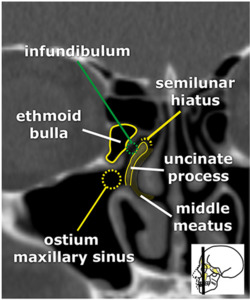
Fig. 4: Coronal CT image.
Osteomeatal unit.
References: R.L. Widya,LUMC, start Radiology
- The spheno-ethmoidal recess drains the posterior third of the bilateral ethmoid and the sphenoid sinuses.
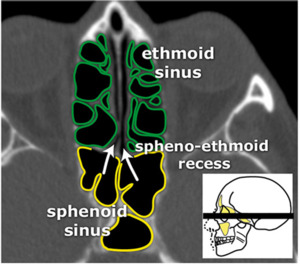
Fig. 5: Axial CT image.
Spheno-ethmoid recess
References: R.L. Widya,LUMC, start Radiology
What should we mention on our report?
It is important to mention the critical anatomical variants of the sinonasal cavities,
in order to warn the otolaryngologist,
helping preoperative planning,
and to prevent serious complications,
particularly haemorrhagic and nervous ones.
Based on a manuscript named 'Avoiding a “CLOSE” Call with Surgical
Complications' (O’Brien et al) proposing the use of the mnemonic “CLOSE” (Cribriform plate, Lamina papyracea,
Onodi cell,
Sphenoid sinus pneumatization,
and (anterior) Ethmoidal artery) wich quickly remind radiologists of these critical variants so that they can be included systematically in the preoperative imaging report.
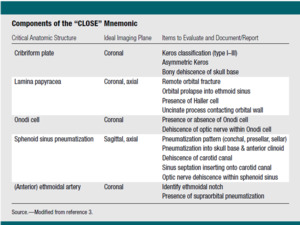
Fig. 6: Components of the “CLOSE” Mnemonic.
References: O’Brien et al,The Preoperative Sinus CT: Avoiding a “CLOSE” Call with Surgical Complications1, adiology.rsna.org,2016
1- Cribriform plate:
- The ethmoid roof: It is of paramount importance because it exposes to a double nerveous and haemorrhagic risk.
First,
it is most vulnerable to iatrogenic cerebro-spinal fluid leakage.
Secondly,
the anterior ethmoid artery may be damaged in per-operative which can cause devastating bleeding in the orbit.
The depth of the olfactory fossa is determined by the height of the lateral lamella of the cribriform plate,
which is part of the ethmoid bone.
It dertermines Keros classification that includes three types:
Keros I:<3mm.
KerosII: 4-7mm.
Keros III:8-16mm : most predisposed to iatrogenic injury.
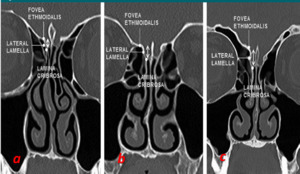
Fig. 7: Coronal CT images.
Keros Classification showing several types depths of the olfactory fossa.
Keros type I (a) defined as less than or equal to 3 mm
in depth - Keros type II (b) defined as a depth of 4–7 mm - Keros type III(c) defined as greater than 7 mm in depth.
References: O’Brien et al,The Preoperative Sinus CT: Avoiding a “CLOSE” Call with Surgical Complications1, adiology.rsna.org,2016
- Bony dehiscence of skull base
2-Lamina papyracea:
-Orbital prolapse into ethmoid sinus

Fig. 8: Coronal CT image.
Right orbital prolapse into ethmoid sinus.
References: O’Brien et al,The Preoperative Sinus CT: Avoiding a “CLOSE” Call with Surgical Complications1, adiology.rsna.org,2016
-Presence of Haller cell: A Haller cell represents an ethmoid air cell that is located lateral to the maxillo-ethmoidal suture along the medial orbital floor,
which narrows the infundibulum.

Fig. 9: Coronal CT image.
Haller cell.
References: R.L. Widya,LUMC, start Radiology
-The uncinate process: Uncinate process contacting orbital wall or reducing the infudibulum.
-The Agger nasi cell: is a named frontal recess cell that represents the most anterior ethmoid air cell.
It has a portion of the anterior margin of the frontal recess and its size may directly influence the patency of the frontal recess and the anterior middle meatus.
3-Onodi cell:
An Onodi cell refers to a spheno-ethmoidal air cell above and lateral to the sphenoid sinus,
placing the optic nerves at risk for intraoperative injury.
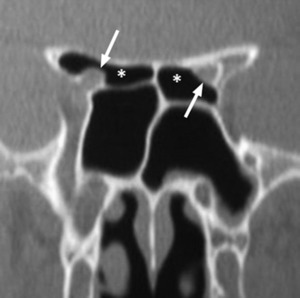
Fig. 10: Coronal CT image.
Bilateral Onodi cells (*) that extend along the superior margin of the sphenoid sinuses.
The optic nerves course through the Onodi cells with a thin
bony margin separating them from the sphenoethmoidal
air cells (arrows).
References: O’Brien et al,The Preoperative Sinus CT: Avoiding a “CLOSE” Call with Surgical Complications1, adiology.rsna.org,2016
4-Sphenoid sinus pneumatization:
-Pneumatization into skull base and anterior clinoid.
-Dehiscence of carotid canal.
-Sinus septation inserting onto carotid canal.
-Optic nerve dehiscence within sphenoid sinus.
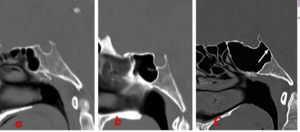
Fig. 11: Sagittal CT images.
Variants of sphenoid sinus pneumatization: chonchal(a),presellar (b) and sellar (c).
The sellar variant results in a thin posterior bony margin of the clivus, which is more susceptible to intraoperative injury
References: O’Brien et al,The Preoperative Sinus CT: Avoiding a “CLOSE” Call with Surgical Complications1, adiology.rsna.org,2016

Fig. 13: Axial and Coronal CT images.
-(a) : Bilateral providence of carotid canals within sphenoid sinus.
-(b) :sphenoid sinus pneumatization extending into the anterior clinoid with resultant exposure of the right optic nerve canal (arrow) within the
sphenoid sinus.
References: O’Brien et al,The Preoperative Sinus CT: Avoiding a “CLOSE” Call with Surgical Complications1, adiology.rsna.org,2016
5-Ethmoidal artery: The anterior ethmoidal arteries are susceptible to intraoperative injury with supraorbital pneumatization of ethmoid air cells (have to be mentionned) above the anterior ethmoidal notch.
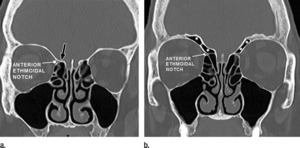
Fig. 12: Coronal reformatted CT images demonstrate the anterior ethmoidal notch along the superolateral margin of the anterior ethmoid sinus.(a) When the ethmoidal notch abuts the fovea ethmoidalis (arrow) or lateral lamella, it is considered protected. (b) With supraorbital pneumatization of the ethmoid sinus above the ethmoid notch (∗), the anterior ethmoidal artery is at risk for intraoperative injury.
References: O’Brien et al,The Preoperative Sinus CT: Avoiding a “CLOSE” Call with Surgical Complications1, adiology.rsna.org,2016
II- Complementarity of CT and MRI couple in the preoperative assessment:
CT retains a place for pre-surgical morphological assessment as well as for the analysis of bone structures of the facial bone and skull base.
However,
it poorly dissociates tumor from inflammatory reactions and poorly analyses the orbital,
perinervous and neuromeningeal extension.
MRI,
with its optimal contrast resolution,
dissociates tumour from soft tissue or adjacent inflammatory phenomena and thus determines the real tumour size (T2 weighted images).
Neuro-meningeal extensions,
at the skull base and at the orbital apex,
major prognostic elements,
are also better evaluated on MRI (multi-plane study T1 and T1 Gadolinium).
It should be noticed that the radiological appearance of benign effusive processes may mimic that of malignant tumors with signs of bone erosions and distant extension such as mucoceles,
aggressive sinusitis...
Histological reminder:
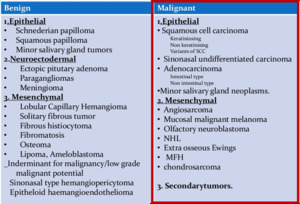
Fig. 14: Table showing several types and subtypes of sinonasal tumors.
References: Dr Durga G: Tumors & tumor like conditions of nasal cavity, Published in Health & Medicine.
As shown in the table above, sinonasal malignant tumors have a several histological types and subtypes and epidermoid ones are the most frequent : epidermoid carcinoma,
adenocarcinoma,
adenoid cystic carcinoma.
Although some radiological signs predict the type of the tumor,
confirmation and histological typing are obtained through biopsy under endoscopic guidance.
Role of imaging
- MRI indication :
-Initial assessment of the tumor : Real tumor size
-Tumoral presentation
-Ways of extension.
-Help with the assessment of operability
-Post-treatment surveillance.
- MRI Protocol:
-Head phased array coils.
-Minimal matrix 256 x352; fields of view :25cm.
-Warn the patient to avoid swallowing,
cough and jerky breathing.
-Sequences:
*T2-weighted series without fat-supression at least two orthogonal T2W planes.
*T1 weighted series without Fat-suppression.
*T1 weighted series Fat-suppressed and injected series (At least 2 orthogonal planes).
*Angio-MR sequence if we suspect vascular tumor.
*Ganglionic sequence (malignant tumor++): Axial series from the base of skull to the sternal manubrium (T2 W or T2 W FAT-SAT+++ or T1W injected).
Initial assessment of the tumor :
- Location and real tumor size:
MRI,
with its optimal contrast resolution,
dissociates the tumour from soft tissue or adjacent inflammatory phenomena and thus determines the real tumour size (T2 weighted images).
Most of the malignant sinonasal tumors present as solid lesion with intermediate signal in T1 and T2 weighted sequences and marked enhancement is usually seen with necrosis stigma.
This is in juxtaposition to predominant T2 hyperintensity related to associated fluid,
retention sinusitis and surrounding inflammation.
However no histological confirmation can be predicted in MRI,
since there are no specific characteristics.
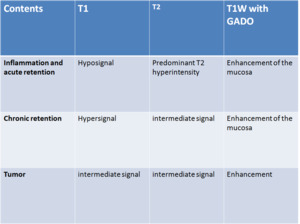
Fig. 15: Sinus content and MRI interpretation
References: DR Jrad M. Höpital Rabta, Tunis/TN.
- Warn the otolaryngologist of risk biopsies:
-Presence of meningocele.
-Meningioma
-Hypervascular tumors
- Assessment of tumor spread:
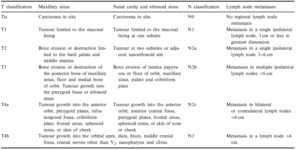
Fig. 16: TN classification of carcinoma of the nasal cavity, ethmoid and maxillary sinuses according to the 7th edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual
References: the American Joint Committee on Cancer (AJCC) Cancer Staging Manual
Computed tomography (CT) and magnetic resonance imaging (MRI) are complementary modalities that demonstrate the potential extension of tumors into adjacent regions that may impact on surgical or therapeutic planning,
particularly when they involve the base of the skull, pterygopalatine fossa,
orbits, nasopharyngeal or palate.
Ways of spread:
- Orbit
The tumor spread by different ways:
-Invasion of the orbital floor (maxillary sinus tumor).
Fig. 17 Fig. 19
-Osteolysis of the lateral ethmoid wall (ethmoïdo-nasal tumor).
-Via nasolacrimal duct (nasal cavity tumor).
-Perineural extension via the superior orbital fissure (V1) or inferior orbital fissure (V2) Fig. 18 ( tumors invading pterygopalatine fossa).
*Modification of the orbit bony walls in contact with the tumor predicts the extension,
such as erosion or osteolysis noticed on CT.
Howerver MRI may detect subtle signal changes in fatty bone marrow (T1 hyperintense) that may herald tumor invasion either by direct geographic spread or perineural extension and which may be completely normal in appearance on CT.
*Invasion of orbital fat or oculomotor muscles.
2.The deep spaces of the face
Invasion of the infratemporal fossa is usually associated with advanced malignancies and a poor prognosis.
Fig. 17 Fig. 18 Fig. 20
-Osteolysis of the posterior wall of the maxillary sinus promotes extension to the maxillo-zygmatic fat space.
-The ethmoid or nasal tumors can invade the infratemporal fossa indirectly through the spheno-palatine foramen and pterygo-palatine fossa (PPF).
Fig. 17
- However,
invasion of deep spaces promotes perineural,
orbital (inferior orbital fissure) tumor dissemination towards the skull base.
3.Oro and nasopharynx:
-Oropharynx extension: concerns usually tumors of the maxillary sinus which erodes the bone of the palate and the dental arch.
Fig. 20
-Naopharynx extension: mainly observed in tumors located in sphenoid sinus responsible in infiltration or lysis of the body of the sphenoid.
4.Endocranial extension: Fig. 23
Endocranial extension is due in a direct way via lysis of the bone sinus walls or indirectly following a perineural invasion.
Dural invasion can not be concluded by linear enhancement alone,
but is certain when dural thickening is more than 5mm or there is pial enhancement or focal dural nodules.
5.
Perineural extension:
This type of extension is correlated with an unfortunate prognosis since it favours distant invasion away from the original tumor site,
endocranial extension and tumor recurrence after treatment.
Adenoid cystic carcinoma and squamous cell carcinomas are usually involved.
It can borrow different ways.
- Maxillary and nasal tumors are the cause of perineural spread into the pterygo-palatine fossa through the infra-orbital nerve (orbital floor),
canals or posterior palatal alveolar nerve (posterior wall of the maxillary sinus).
Fig. 17 Fig. 18
- Nasal or ethmoid tumors which come in contact with the cribriform plate spread along the olfactory nerve .
FPP involvement presents an evolutionary turning point in tumor progression since it presents a perineural extension path.
It puts in communication nasal cavity,
masticator space,
orbit,
middle cranial fossa and delivers passage to the V2 nerve.
Thus, it promotes the extension to the orbital apex (via V2 )and into the cavernous sinus through the orbital fissure and round foramen.
What signs predicting perineural extension ?
- Enlargement or osteolysis of formens.
- Loss of the perineal hypersignal.
- Perinervous or nerve enhancement after injection.
To summarize,
these several ways of spread have to be consistently evaluated and documented on our preoperative imaging report.
In fact,
computed tomography (CT) and magnetic resonance imaging (MRI) are complementary modalities that excel at demonstrating the location and overall size of such masses and their potential extension into adjacent regions that may impact on surgical or therapeutic planning.
Radiologist must be familiar with the therapeutic management of these tumors,
which largely depends on the radiological report.
To simplify;
-T1,
T2 and T3: Surgery.
-T4a Moderately advenced : surgery is discussed.
-T4b Very advanced : No surgery +++ Fig. 23
- Important endocranial extension.
- Extension to the orbital apex.
- Perineural extension.
- Invasion of the cavernous lodge.
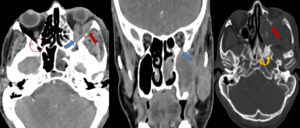
Fig. 18: Same patient.
Axial and coronal CT images with soft tissue window show an abnormal enlargement and ivasion of the inferior orbital fissure (Blue arrow) [compared to the contralateral side (Red circle)] which presents a way of spread to the floor of the orbit.
CT image with bone windows shows the coexistence of osteolysis and bone sclerosis : destruction of sinus walls and the lateral orbital wall (Red arrow) associated to the bone sclerosis of the pterygoid plate (Yellow star).
In fact CT has a key role in the analysis of bone structures.
References: Hôpital Charles Nicolle-Tunis
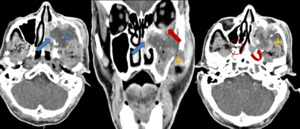
Fig. 17: 72 years old patient followed for squamous cell carcinoma of the left maxillary sinus. Contrast-enhanced CT images showing an ill-demarcated, heterogeneously enhanced bulky mass with areas of necrosis included (blue star). The tumor medially extends into nasal fossa (Blue arrow) and invades superiorly the floor of the orbit through extensive bone lysis (Red arrow). It has an intimate contact with the inferior rectus muscle (Red arrow) however it is difficult on CT to confirm its invasion (an additional MRI study is necessary). The tumor destroys the posterior wall of the sinus and invades pterygopalatine fossa PPF (curved arrow) [compared to the contralateral side where PPF is free (Red circle)]. There is infiltration of the retroantral fat and masseter muscle consistent with spread into the infratemporal fossa (Yellow star).
References: Hôpital Charles Nicolle-Tunis
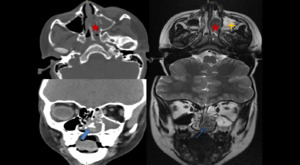
Fig. 21: CT images with bone window show a mass filling right nasal cavity and maxillaty sinus with osteolysis of medial sinus wall and middle nasal concha(Red star) associated to a calcification within the meatus.
Both fungal sinusitis and tumoral process were evocated and we have completed with an MRI.
Axial and coronal T2 Weighted images show relatively homogeneous, intermediate signal mass (Red star) of the nasal cavity with hypersignal T2 foci (Blue arrow) corresponding to the calcifications.
Trapped secretions are associated within maxillary sinus (Yellow star).
References: Hôpital Charles Nicolle-Tunis

Fig. 22: Same patient.
Coronal(a) and axial(b) T1 Weighted Fat suppressed and injectid images show the mass described above with no enhancement. However peripheral and regular enhancement is noted consistent with obstructed secretions and surrounding mucosal thickening.
The diagnosis of sinusitis was rather restrained
References: Hôpital Charles Nicolle-Tunis
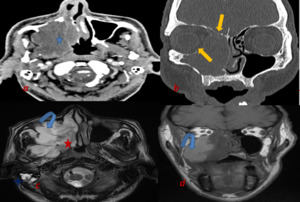
Fig. 19: Axial CT image (a) shows a large soft tissue heterogeneous mass filling the right maxillary sinus with extension to the nasal cavity and infra-temporal fossa.
It is difficult on CT to distinguish antral tumor extension from obstructed secretions.
Coronal CT image with bone window shows osteolysis of the medial orbital wall and of the ethmoid roof.
Orbital and meningeal extension should be sought and an additional MRI study is necessary.
Axial T2 Weighted MR image (c) shows the mass filling nasal cavity and locally aggressive in intermediate hypersignal (Red star) with areas showing characteristic curvilinear or “cerebriform” architecture witch is evocateur of inverted papilloma. MRI dissociate the tumor from obstructed secretions (Blue curved arrow)at the maxillary sinus that appear in hypersignat T1 and T2 and consistent with chronic retention.
An associated retention into mastoid cells in hypersignal T2 (Blue star).
References: Hôpital Charles Nicolle-Tunis
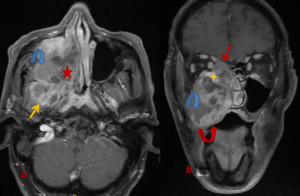
Fig. 20: Same patient.
Axial(a) and coronal (b) T1 Weighted images fat suppressed and injected show the mass of the nasal cavity and the maxillary sinus with heterogeneous enhancement and areas of necrosis included.
It spreads into the infratemporal fossa and infiltrates masticator space and ptérygoid muscles (Yellow arrow).
Coronal MR image shows cephalad extension of the mass through the floor of the orbit, the invasion of extraconal space and ints contact with inferior rectus muscle (yellow arrow).
Superiorly, it invades ethmoidal cells and cribriform plate without dural invasion(Red arrow). Inferiorly tumor erodes the bone of the palate, the dental arch and spreads into the oropharynx.
Histological result: inversed papilloma associated with synchronous squamous cell carcinoma.
References: Hôpital Charles Nicolle-Tunis
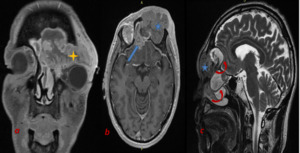
Fig. 23: 63 years old patient followed for squamous cell carcinoma of the left frontal sinus.
Coronal(a) and axial(b) T1 Weighted fat suppressed and injected images.
Sagittal T2 Weighted MR image (c).
Ill-demarcated, heterogeneously enhanced mass with necrosis stigmas within right frontal sinus and homolateral ethmoid (arrow).Coronal post-contrast MRI image highlights invasion across the skull base and cribriform plate into the anterior cranial fossa (Blue arrow).
Obstructed secretions associated (Red curved arrow).
Since the tumor presents significant intracranial extension and spreads into orbital apex (Yellow star), it is classified T4b (No surgery).
References: Hôpital Charles Nicolle-Tunis


. The tumor medially extends into nasal fossa (Blue arrow) and invades superiorly the floor of the orbit through extensive bone lysis (Red arrow). It has an intimate contact with the inferior rectus muscle (Red arrow) however it is difficult on CT to confirm its invasion (an additional MRI study is necessary). The tumor destroys the posterior wall of the sinus and invades pterygopalatine fossa PPF (curved arrow) [compared to the contralateral side where PPF is free (Red circle)]. There is infiltration of the retroantral fat and masseter muscle consistent with spread into the infratemporal fossa (Yellow star). References: Hôpital Charles Nicolle-Tunis")
 shows a large soft tissue heterogeneous mass filling the right maxillary sinus with extension to the nasal cavity and infra-temporal fossa.
It is difficult on CT to distinguish antral tumor extension from obstructed secretions.
Coronal CT image with bone window shows osteolysis of the medial orbital wall and of the ethmoid roof.
Orbital and meningeal extension should be sought and an additional MRI study is necessary.
Axial T2 Weighted MR image (c) shows the mass filling nasal cavity and locally aggressive in intermediate hypersignal (Red star) with areas showing characteristic curvilinear or “cerebriform” architecture witch is evocateur of inverted papilloma. MRI dissociate the tumor from obstructed secretions (Blue curved arrow)at the maxillary sinus that appear in hypersignat T1 and T2 and consistent with chronic retention.
An associated retention into mastoid cells in hypersignal T2 (Blue star). References: Hôpital Charles Nicolle-Tunis")
 [compared to the contralateral side (Red circle)] which presents a way of spread to the floor of the orbit.
CT image with bone windows shows the coexistence of osteolysis and bone sclerosis : destruction of sinus walls and the lateral orbital wall (Red arrow) associated to the bone sclerosis of the pterygoid plate (Yellow star).
In fact CT has a key role in the analysis of bone structures. References: Hôpital Charles Nicolle-Tunis")
 and coronal (b) T1 Weighted images fat suppressed and injected show the mass of the nasal cavity and the maxillary sinus with heterogeneous enhancement and areas of necrosis included.
It spreads into the infratemporal fossa and infiltrates masticator space and ptérygoid muscles (Yellow arrow).
Coronal MR image shows cephalad extension of the mass through the floor of the orbit, the invasion of extraconal space and ints contact with inferior rectus muscle (yellow arrow).
Superiorly, it invades ethmoidal cells and cribriform plate without dural invasion(Red arrow). Inferiorly tumor erodes the bone of the palate, the dental arch and spreads into the oropharynx.
Histological result: inversed papilloma associated with synchronous squamous cell carcinoma. References: Hôpital Charles Nicolle-Tunis")
 and axial(b) T1 Weighted fat suppressed and injected images.
Sagittal T2 Weighted MR image (c).
Ill-demarcated, heterogeneously enhanced mass with necrosis stigmas within right frontal sinus and homolateral ethmoid (arrow).Coronal post-contrast MRI image highlights invasion across the skull base and cribriform plate into the anterior cranial fossa (Blue arrow).
Obstructed secretions associated (Red curved arrow).
Since the tumor presents significant intracranial extension and spreads into orbital apex (Yellow star), it is classified T4b (No surgery). References: Hôpital Charles Nicolle-Tunis")
 associated to a calcification within the meatus.
Both fungal sinusitis and tumoral process were evocated and we have completed with an MRI.
Axial and coronal T2 Weighted images show relatively homogeneous, intermediate signal mass (Red star) of the nasal cavity with hypersignal T2 foci (Blue arrow) corresponding to the calcifications.
Trapped secretions are associated within maxillary sinus (Yellow star). References: Hôpital Charles Nicolle-Tunis")