1.
ANATOMICAL REVIEW
A thorough knowledge of Mediastinal Anatomy and the possible pathways of infection spreading from adjacent sites is basic to understand the pathophysiology of the different types of acute mediastinitis.
Fig. 1
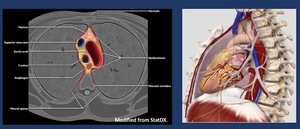
Fig. 1: The laxity of the mediastinal sof tissue allows the infection to progress rapidly. However, both pleuras (Red Lines) surrounding the mediastinum ( act as a barrier containing the infection (A).
This barrier–effect delays the spreading to the lungs, but at the same time generates a close-space abscess in such a highly dangerous anatomic area with many vital organs such as the heart, the great vessels, the trachea or the esophagus (B).
References: STATDX/MODIFIED
The mediastinum extends from the thoracic inlet superiorly to the diaphragm inferiorly and from the sternum anteriorly to the thoracic vertebrae posteriorly.
1.1.-Felson´s classification of Mediastinal spaces, based on arbitrary landmarks outlined on the lateral chest radiograph Fig. 2 has been widely used.
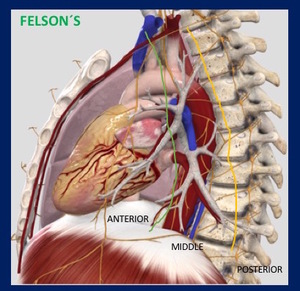
Fig. 2: Felson´s Mediastinal Compartments
1.2.- A new scheme based on cross-sectional imaging,
principally multi- detector computed tomography (CT),
has been developed by the International Thymic Malignancy Interest Group (ITMIG) and accepted as a new standard.
This clinical division scheme defines unique prevascular,
visceral,
and paravertebral compartments based on boundaries delineated by specific anatomic structures at multidetector CT.
Table 1 .
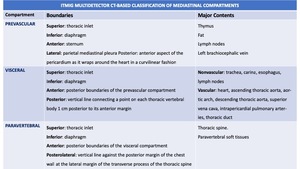
Table 1: ITMIG Mediastinal Cross Sectional CT Mediastinal Compartments
The prevascular compartment (purple) wraps around the heart and pericardium,
which are located in the visceral compartment (blue).
Yellow = paravertebral compartment,
green line = visceral-paravertebral compartment boundary line Fig. 3 .
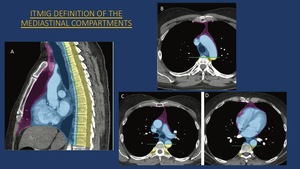
Fig. 3: ITMIG Mediastinal Compartments Pictorial Scheme
References: RADIOGRAPHICS
1.3.-MEDIASTINUM CONTENTS
Organs
- Thymus
- Heart
- Aerodigestive tract
- Trachea and proximal mainstem bronchi
- Esophagus
Vessels
- Systemic arteries
- Thoracic aorta and branches
- Systemic veins
- Venae cavae,
azygos,
and hemiazygos systems
- Pulmonary vessels
- Central pulmonary arteries and pulmonary veins
Lymphatics,
thoracic duct,
lymph nodes
Nerves
- Vagus nerves (cranial nerve X)
- Right vagus nerve courses inferiorly along lateral trachea,
behind hilum,
and along lateral esophagus
- Left vagus nerve courses inferiorly along lateral aortic arch,
behind hilum,
and along lateral esophagus
- Left recurrent laryngeal nerve: Branch of left vagus nerve at lateral aortic arch,
courses under aortic arch,
and continues superiorly toward neck in groove between trachea and esophagus to supply larynx
- Phrenic nerves
- Right phrenic nerve is lateral to vagus nerve,
courses along lateral aspect of right brachiocephalic vein,
continues anterior to hilum along lateral pericardium
- Left phrenic nerve is lateral to vagus nerve and proximal left brachiocephalic vein,
courses along lateral proximal aortic arch,
and continues anterior to hilum along lateral pericardium
Mesenchymal tissues
Pericardium
Mediastinal fat
2.
CLINICAL SIGNS
The Clinical Symptoms of Acute Mediastinits may include some of the following:
- Acute Chest Pain (retro-sternal/inter-scapular)
- High fever,
chills,
shortness of breath,
and leukocytosis
- Dysphagia,
Sore throat
- Neck swelling/subcutaneous emphysema
- Pleural Effusion/empiema
- Pre-sternal skin erytema Fig. 5
In a review of the literature,
the above mentioned signs are found in different percentages in patients diagnosed of Acute mediastinitis.
Increased attenuation of mediastinal fat is found in almost 100% of the cases.
Localized mediastinal fluid collections were founfd in 55% of the cases; free gas bubbles in the mediastinum in 57%; mediastinal lymph nodes in 35%; pericardial effusions in 27%; pleural effusions in 85%; lung infiltrates in 35%; sternal dehiscence in 40% and pleuropulmonar fistula in 2,5%.
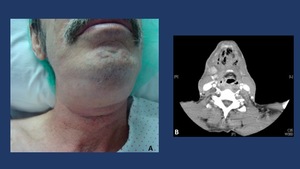
Fig. 5: Sore throat, neck swelling, fever, and skin erythema are clinical signs/symptoms of a deep neck infection. The persistence of the symptoms and the downward progression of the different signs must warn the clinician of the possible development of a descending necrotizing mediastinitis. In these situations a CT scan, when available, is mandatory to assess the severity and extension of the infection process.
3.
IMAGING TECHNIQUES
3.1.- Chest radiography is the first imaging examination that is performed to evaluate patients with suspected nonvascular,
nontraumatic mediastinal emergencies.
Both anteroposterior and lateral views of the chest are obtained.
Findings seen at chest radiography are considered diagnostic in patients with pneumomediastinum or pneumopericardium,
although it may be dificult to identify a tension component of these conditions at radiography.
Fig. 6

Fig. 6: Chest radiography is the first imaging examination that is performed to evaluate patients with suspected nonvascular, nontraumatic mediastinal emergencies. Both anteroposterior and lateral views of the chest are obtained. Pneumomediastinum or pneumopericardium are considered high suspicion findings of Acute Mediastinitis.
3.2.-Neck radiography may depict subcutaneous emphysema,
prevertebral soft-tissue swelling,
mediastinal air,
and widening of the superior mediastinum
In addition to mediastinal air and fluid collections,
neck CT findings of DNM include thickening of the subcutaneous tissues in the neck,
thickening or enhancement of cervical fascia and muscles, fluid collections,
and enlarged lymph nodes.
Fig. 7

Fig. 7: A: Lateral Neck x-Ray Neck radiography may depict subcutaneous emphysema, prevertebral soft-tissue swelling (Arrow), mediastinal air (*), and widening of the superior mediastinum. B: Good correation with the CT findings in a sagital MPR reconstruction, with high density material perforating the posterior aspect of the middle third of the esophagus. Surgical specimen prove to be a chicken bone.
3.3.-Contrast esophagography is indicated in patients with sus- pected IHE,
esophageal perforation,
or esophagorespiratory fistula.The use of hydrosoluble contrast material is preferred over barium in these patients,
and computed tomography (CT) is the imaging modality of choice.
3.4.-CT
CT is the imaging modality of choice.
It is readily available,
rapid,
noninvasive,
easy to perform,
and useful in detecting various mediastinal emergencies.
The sensitivity and specifity of CT in postopertaive patients in the first 15 dyas after surgery is almost 100% and 30 % respectively,
and after the first two weeks,
almost 100% and 90% respectively.
In patients with Descending Necrotizing Mediastinitis,
sensitivity was 90-100% while in patients with suspected esophageal perforation,
sensitivity and specifity were superior to 90%.
In a typical CT protocol for evaluating mediastinal conditions,
1.5-mm section thickness and 3-mm reconstruction intervals are used at 140 kvp and 160 mA.
Intravenous contrast material is routinely used because many patients present with chest pain,
and vascular pathologies are often suspected.
For the enhanced series is suggested a volume of 100 ml of non-ionic contrast media injected at a rate of 2 ml/s,
scan delay time of 30s.
When Descending Necrotizing Mediastinitis is suspected,
the region covered should extend from the skull base to the dome of the diaphragm.
The use of oral contrast material is recommended in patients suspected of having esophageal conditions.
3.5.-Common CT FINDINGS in ACUTE MEDIASTINITIS (AM) Fig. 8 :
- Increased attenuation of mediastinal fat
- Free gas bubbles in the mediastinum
- Localized fluid collections
- Enlarged lymph nodes
- Pleural effusions /Empyema
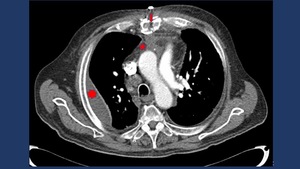
Fig. 8: CT findings in AM include among others: pleural effusion (*), mediastinal fat stringiness (star) and free air bubbles.
4.- MAIN CAUSES OF ACUTE MEDIASTINITS
Acute Inflammation of the mediastinum may have several causes. The three main groups include postoperative cardiothoracic surgery,
esophageal perforation (Boerhaave's syndrome,
dilatations,
foreign bodies,
etc.),
as well as head and neck deep infections spreading to the mediastinum such as peritonsillar abscesses,
odontogenic cervical abscesses,
Ludwig angina,
etc. ) Other less common causes include pleural empyema,
hematogenous spreading,
osteomyelitis of the sternoclavicular joint ( in patients addicted to iv drugs) vertebrae and ribs,
retroperitoneal abscesses and subphrenic abscesses.
We will now focus on the three main groups of causes of Acute Mediastinits (FIG.8) Table 2 :
- Postoperative infection.
- Esophageal Perforation
- Descending Necrotizing Mediastinitis.

Table 2: Main Etiologies of Acute Mediastinitis.
4.1.- Postoperative Infections
Time dependence of CT accuracy in postoperative patients is related to the fact that normal postoperative appearances of the mediastinum during the first 2–3 weeks are quite similar to mediastinitis and may not return to normal for as long as 2 months after surgery.
Increased attenuation of mediastinal fat was recorded in all of our patients,
but does not seem to be a specific finding in the postoperative group of patients during the first 3 weeks.
Gas bubbles in the mediastinum with or without associated fluid collections are found in up to half of the reported mediastinitis series However,
gas bubbles and mediastinal fluid colections may be normal findings for at least 21 days after surgery,
and are observed in more than 75% of asymptomatic patients.
These difficulties have been considered a significant drawback of CT and have led some authors to infer that CT has limited usefulness in the diagnosis of postoperative complications.
Persistence of these findings after 15 dyas postoperatively ,
however,
is highly indicative of mediastinitis.
Correlation with other clinical and laboratory results further increases diagnostic yield.
CT findings in Postoperative Infections include,
besides common CT findings in AM:
- Sternum Dehiscence
- Displacement,
rotation and fracture of the sternal wires
- Midsternal lucent stripe>3mm in CT
- Mediastinal gas bubbles and fluid collections on CT images after the 14th postoperativeday has sensitivity and specificity approaching 100% for the diagnosis Fig. 9 .
Differential diagnosis of loculated fluid collections includes seromas which lack wall contrast enhancement.
However,
fluid collections of mediastinitis may not present enhancement if presented within 1 week postoperatively.
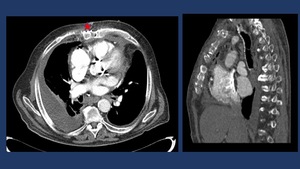
Fig. 9: CT-enhanced in AM post Cardiac Surgery. Skin to mediastinum fistulae and sternal radiolucent strip >3 mm (star).
4.2.- Esophageal Rupture
Esophageal perforation is a life threatening condition that may rapidly progress to fulminant mediastinitis and septic shock and is associated with Boerhaaves’ syndrome,
iatrogenic trauma and cancer of the esophagus Early diagnosis of esophageal perforation allows prompt in- stitution and appropriate medical and surgical intervention In some series,
mediastinitis developed in almost 57% of the patients who were referred to the CT department.
Prompt recognition is crucial; in most studies a delay in diagnosis and treatment beyond 24 h adversely affects prognosis CT scan assists in early diagnosis and provides information concerning the extent of pathology.
Patients who developed mediastinitis following esophageal perforation usually presented findings of free mediastinal gas,
fluid collections and increased mediastinal fat density as early as in the first 24h. Esophagopleural fistula is a specific finding demon- strating extraluminal leak,
but is not commonly seen.
CT findings of Esophageal Rupture include focal esophageal Wall thickening,
periesophageal fluid collections,
free mediastinal air,
and contrast extravasation into the mediastinum and pleural space.
Fig. 10
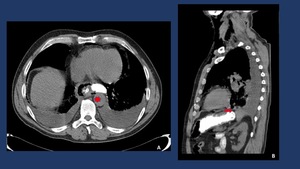
Fig. 10: CT-non enhanced with oral contrast showing contrast leakage in the left-inferior aspect of the esophagus in a patient diagnosed of a Boerhaave Syndrome.
Perforation in the superior two thirds of the esophagus is usually due to foreign bodies ingestion.
In the lower third,
the main causes are iatrogenic and the Boerhaave Syndrome.
Boerhaave syndrome is an spontaneous perforation of the esophagus most commonly resulted from a full-thickness tear in the esophageal wall due to a sudden increase in intraesophageal pressure combined with relatively negative intrathoracic pressure caused by straining or vomiting .
In most cases of Boerhaave's syndrome,
the tear occurs at the left postero-lateral aspect of the distal esophagus and extends for several centimeters. Mackler's triad includes chest pain,
vomiting,
and subcutaneous emphysema,
and while it is a classical presentation,
it is only present in 14% of people.
The condition is associated with high morbidity and mortality and is fatal without early treatment.
Fig. 11
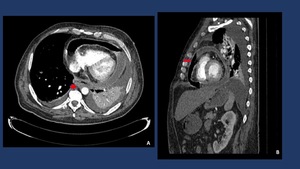
Fig. 11: CT-contrast enhanced depicts a massive pneumopericardium secondary to an esophageal-pericardium fistula in a patient with an epidermoid esophageal cancer.
4.3.-Necrotizing Descending Mediastinitis
Acute descending necrotizing mediastinitis is an acute rapidly progressive polymicrobial infection of the mediastinum with reported mortality rates ranging from 30 to 50%. The spread of the infection has been attributed to dependent drainage from the neck into the mediastinum,
negative intrathoracic pressure,
and synergistic bacterial growth.
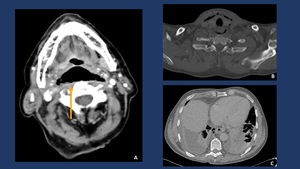
Fig. 12: Descending spread of inflammation along the retrovisceral space (“danger zone”) to the posterior mediastinum from a retropharyngeal abscess. Diagnosis was confirmed by surgery.
The deep cervical fascia of the neck is composed of a superficial,
a visceral and a prevertebral layer,
which create the retrovisceral and prevertebral spaces respectively,
also named the “danger zone”,
through which infectious material can dissect from the deep neck soft tissues to the mediastinum.
Another pathway of infection spread is through the carotid sheath down into the upper mediastinum,
also described as “Lincoln’s Highway”.
Each of these potential spaces contains loose areolar tissue and readily serves as a site of entry of an oropharyngeal or cervical infection into the chest .
Due to the increased mortality,
despite modern antimicrobial therapy,
several authors recommend that CT should be performed early,
since it may identify pathology at a time when chest X-rays are still unremarkable
Computed tomography is considered the diagnostic modality of choice in DNM,
because it clearly delineates the location and extent of the pathology,
assists in clinical decision regarding which patients require immediate surgical intervention and which can be managed conservatively demonstrates associated pleural and parenchymal disease,
and also evaluates the success of treatment on follow-up scans.
In addition to mediastinal air and fluid collections,
neck CT findings of DNM include thickening of the subcutaneous tissues in the neck,
thickening or enhancement of cervical fascia and muscles, fluid collections,
and enlarged lymph nodes.
Fig. 12
Endo CT Classification Table 3 is basic to evaluate the need for a surgical drainage Fig. 13 .
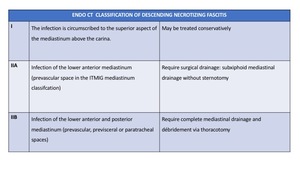
Table 3: Endo´s Classification of Descending Necrotizing Mediastinitis.

Fig. 13: A. Intraoperative view of the purulent drainage from a cervical abscess. B. Inmediate Postoperative view of a DNM showing a Tracheostomy and multiple drains throughout the floor of the mouth, the neck and the mediastinum.
Knowledge of the different ways of spreading from deep neck infections to mediastinum is vital to determine the origin of the infection and the possible complications.
Special attention should be made to a possible extension to the retropahryngeal "danger space" as it allows infections to track downward to the level of the mediastinum.
This can result in mediastinitis,
empyema,
and sepsis.
Fig. 14 Fig. 15
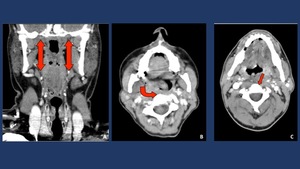
Fig. 14: Deep Neck infections may spread through the parapharyngeal space (“elevator shaft”). A. Normal parapharyngeal space (PPS). B Phlegmon extending from the right masticator space to the PPS. C. Phlegmon extending form the pharyngeal mucosal space to the retropharyngeal space.
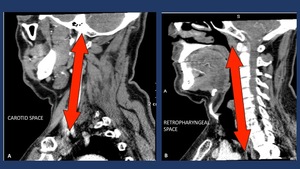
Fig. 15: There are three potential pathways for the spread of infection from the neck to the mediastinum: the pretracheal route
to the anterior mediastinum, the lateral pharyngeal route to the middle mediastinum, including the carotid space or ”Linconl´s Highway) (A), and the retropharyngeal-retrovisceral route to the posterior mediastinum (B). Of these, the most common route is by way of the retropharyngeal-retrovisceral space

 surrounding the mediastinum ( act as a barrier containing the infection (A).
This barrier–effect delays the spreading to the lungs, but at the same time generates a close-space abscess in such a highly dangerous anatomic area with many vital organs such as the heart, the great vessels, the trachea or the esophagus (B).
References: STATDX/MODIFIED")






, mediastinal air (*), and widening of the superior mediastinum. B: Good correation with the CT findings in a sagital MPR reconstruction, with high density material perforating the posterior aspect of the middle third of the esophagus. Surgical specimen prove to be a chicken bone.")
, mediastinal fat stringiness (star) and free air bubbles.")

.")



 to the posterior mediastinum from a retropharyngeal abscess. Diagnosis was confirmed by surgery.")

. A. Normal parapharyngeal space (PPS). B Phlegmon extending from the right masticator space to the PPS. C. Phlegmon extending form the pharyngeal mucosal space to the retropharyngeal space.")
 (A), and the retropharyngeal-retrovisceral route to the posterior mediastinum (B). Of these, the most common route is by way of the retropharyngeal-retrovisceral space")