ECR 2019 / C-3508
Adenomyosis and MRI
Congress:
ECR 2019
Poster Number:
C-3508
Type:
Educational Exhibit
Keywords:
Pelvis, Genital / Reproductive system female, Anatomy, MR, Ultrasound, CT, Education, Image compression, Perception image, Hyperplasia / Hypertrophy, Cysts, Dilatation
Authors:
J. Murillo1, D. STOISA2, R. L. Villavicencio2; 1Tegucigalpa, FM/HN, 2Rosario/AR
DOI:
10.26044/ecr2019/C-3508

Fig. 1

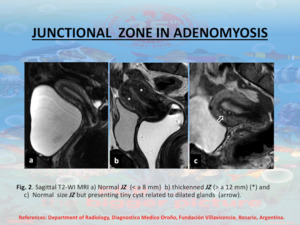
Fig. 2

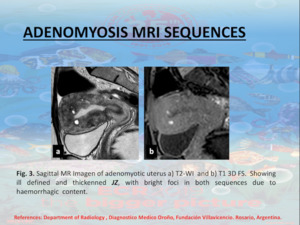
Fig. 3

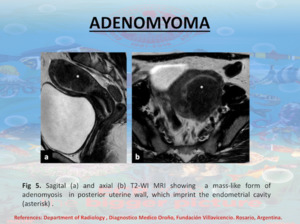
Fig. 5

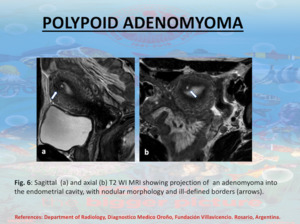
Fig. 6

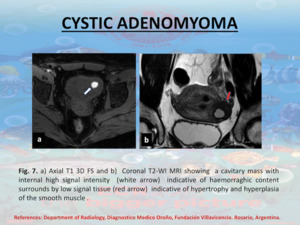
Fig. 7

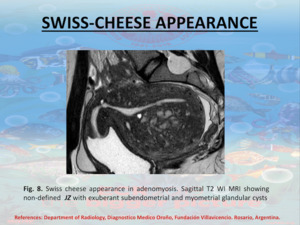
Fig. 8

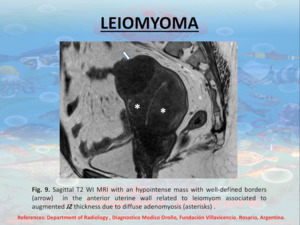
Fig. 9

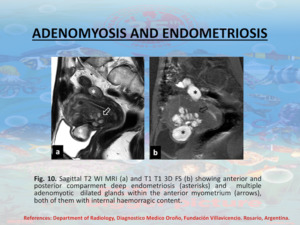
Fig. 10