ECR 2019 / C-3519
Rare idiopathic interstitial pneumonias – radiologic findings and pathologic correlations
Congress:
ECR 2019
Poster Number:
C-3519
Type:
Educational Exhibit
Keywords:
Pathology, Occupational / Environmental hazards, Inflammation, Education, Diagnostic procedure, CT-High Resolution, Conventional radiography, Thorax, Lung
Authors:
M. N. C. D. Silva1, A. T. Vilares2, C. Sousa1, A. Carvalho1, M. S. C. Rodrigues1, R. Cunha1, S. Guimarães1; 1Porto/PT, 2Espinho/PT
DOI:
10.26044/ecr2019/C-3519
 and in a 72-year-old man (C). Postero-anterior radiographs (A,C) show a bilateral reticular pattern in the upper lung zones, with volume loss suggested by upward hilar retraction (yellow arrows). In a magnified image (B) of the right lung upper-third in A, a small chamber of pneumothorax is seen (blue arrow). References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 3:
Biopsy-proven PPFE in a 54-year-old woman (A,B) and in a 72-year-old man (C)....
 and axial (C) CT images show bilateral upper lobe irregular pleural thickening and subpleural reticulation compatible with PPFE. As incidental finding, in the lower lobes, specially on the left lung, some peripheral ground-glass centrilobular nodules are seen, with “tree-in-bud” distribution, compatible with bronchiole filling by bacterial bronchopneumonia. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 4:
Biopsy-proven PPFE in a 65-year-old female patient. Coronal (A,B) and axial (C)...
 and in a 50-year-old man (B). Coronal (A,B) CT images show the characteristic bilateral upper lobe irregular pleural thickening and subpleural reticulation. Some associated cystic bronchiectasis are seen in A and a centrilobular micronodular pattern is seen in B, consistent with concomitant pulmonary involvement by silicosis. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 5:
Biopsy-proven PPFE in a 73-year-old man (A) and in a 50-year-old man (B)....
. Added to the classic pleural thickening, some architectural distortion is seen, with traction bronchiectasis (yellow arrows). Mild paraseptal and centrilobular emphysema is also observed. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 6:
Biopsy-proven PPFE in a 63-year-old female patient (A – axial CT image; B-...
. Severe fibrotic architectural distortion is identified, with upper lobe volume loss, upward hilar retraction and tracheomegaly. Multiple diffuse traction bronchiectasis are seen, predominantly and more severe in the upper lobes. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 7:
Biopsy-proven PPFE in a 71-year-old male (A – axial CT image; B- coronal CT...
. Added to the bilateral pleural thickening, some subpleural cysts are shown in both upper lungs (yellow arrows). Mild paraseptal and centrilobular emphysema. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 8:
Biopsy-proven PPFE in a 65-year-old male (A – axial CT image; B- coronal CT...
. In B, reticular subpleural opacities are identified in regions distal to the pulmonar apices, with mild honeycombing, which raises the possibility of coexistant interstitial involvement (UIP-like pattern).
References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 9:
Biopsy-proven PPFE in a 69-year-old woman (A – axial CT image of the apices;...
, with abundant interstitial elastic fibers (highlighted with orcein in B) enclosing airspaces obliterated by looser connective tissue.
References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 10:
A - Lung biopsy shows distortion of architecture by homogeneous, dense fibrosis...

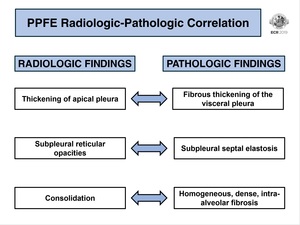
Fig. 11:
PPFE radiologic-pathologic correlation.

Fig. 12:
PPFE differential diagnosis. A- postero-anterior radiograph shows bilateral...
 of two distinct patients with LIP, show a reticular pattern bilaterally, predominantly in the lower lung zones (B). References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 13:
Postero-anterior radiographs (A,B) of two distinct patients with LIP, show a...
. Patchy ground-glass opacities are seen, some appearing centrilobular. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 14:
Biopsy-proven LIP in a patient with Sjögren’s syndrome (A,B,C – axial CT...
. Multiple ill-defined nodules of varying sizes are observed, with peribronchovascular distribution. Few areas of heterogeneous parenchymal attenuation, compatible with mosaic perfusion. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 15:
Biopsy-proven LIP in a patient with common variable immunodeficiency (A,B,C,D...

Fig. 16:
Biopsy-proven LIP in a HIV-positive patient. HRCT show small, well-defined...
. Clustered and dispersed cysts are observed in both upper lobes, some with subpleural distribution. The cystic involvement in the bases is scarse, which is unusual in honeycombing. Discrete interlobular septal thickening is visible in B. References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 17:
Biopsy-proven idiopathic LIP (A– axial CT image at the level of the carina,...
. As this finding is atypical for LIP, the pathologic diagnosis did not match the radiologic, so a second surgical biopsy was recommended. The second histologic evaluation was consistent with LIP.
References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 18:
2-biopsy-proven LIP in a patient with scleroderma. A focal area of...
; rare plasma cells, some histiocytes and macrophages are also present. The lymphoid population is polyclonal.
References: Department of Radiology, Centro Hospitalar de São João - Porto/PT")
Fig. 19:
Moderate lymphocytic inflammatory infiltration with lymphoid follicles with...

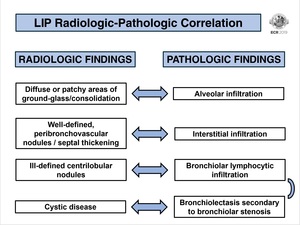
Fig. 20:
LIP radiologic-pathologic correlation.

Fig. 21:
LIP differential diagnosis. A – hypersensitivity pneumonia. Geographic areas...