ECR 2019 / C-3526
Hypovascular pancreatic mass: not only adenocarcinoma
Congress:
ECR 2019
Poster Number:
C-3526
Type:
Educational Exhibit
Keywords:
Tissue characterisation, Education and training, Decision analysis, Ultrasound, MR, CT, Pancreas, Oncology, Abdomen
Authors:
G. Carpani1, R. Cannella2, M. Dimarco2, D. Giambelluca2, M. Midiri2; 1Bologna/IT, 2Palermo/IT
DOI:
10.26044/ecr2019/C-3526

Fig. 3
 in the pancreatic head. References: Department of Radiology, AOUP Paolo Giaccone, University of Palermo / Italy 2018")
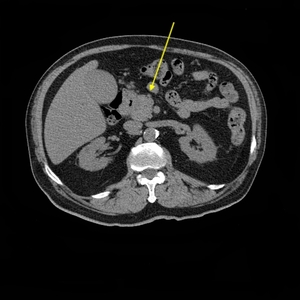
Fig. 4:
56-year-old woman accessing the ER for abdominal pain, with high hepatic...
 in same patient with pancreatic head mass. Not showed: hydropic gallbladder, hepatic metastasis. References: Department of Radiology, AOUP Paolo Giaccone, University of Palermo / Italy 2018")
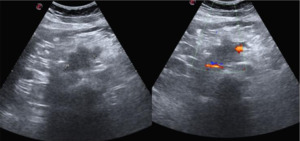
Fig. 5:
Trans-abdominal US associated dilatation of common bile duct (ø 1,5 cm) in...

Fig. 6

Fig. 7

Fig. 8:
72-year-old man presenting with abdominal pain, dysphagia and weight loss....

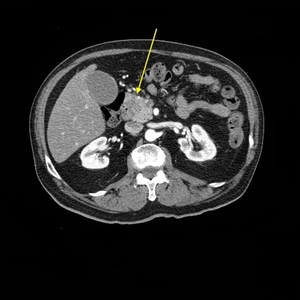
Fig. 9:
Axial CT pancreatic late arterial phase, hypodense lesion of pancreatic head,...

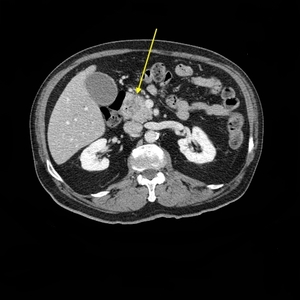
Fig. 10:
Axial CT, portal venous phase, hypodense PDAC of pancreatic head.

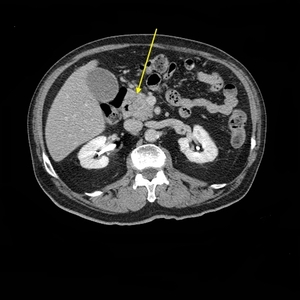
Fig. 11:
Axial CT, delayed phase, inhomogeneous hypodense PDAC of the pancreatic head.
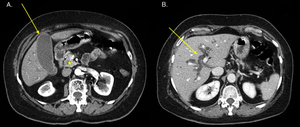
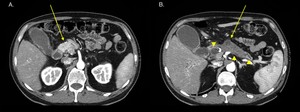
 Hypodense small mass (ø 1,5 cm) of the head of the pancreas (star), associated with indirect signs: hydropic gallbladder. (B) Dilatation of intrahepatic biliary tracts, due to tightened stenosis of common bile duct. Underwent Whipple procedure, biopsy-proven. References: Department of Radiology, AOUP Paolo Giaccone, University of Palermo / Italy 2018")
Fig. 12:
70-year-old woman, presenting whit jaundice and elevated liver function tests....
 Hyperdense pancreatic head parenchima, hydropic gallbladder. (B) Indirect signs of PDAC: atrophic pancreatic tail, dilatation of main pancreatic duct (arrow, arrowhead), dilatation of common bile duct (arrowhead). References: Department of Radiology, AOUP Paolo Giaccone, University of Palermo / Italy 2018")
Fig. 13:
60-year-old man presenting with jaundice and dysphagia.
Axial CT, pancreatic...

Fig. 14

Fig. 15