LIMITS OF THE FIGO CLASSIFICATION
• Clinical classification (Intravenous-urography,
cystoscopy,
rectoscopy…)
• Does not include ganglionic extension
• Poor correlation to surgical findings
Stade I Stade II Stade III
Concordance 68-80% 25-55% 10-50%
5-year survival 95% 65% 41%
ROLE OF IMAGING
ü Tumor size
ü Vaginal and stromal extension
ü Extension to parametria
ü Parietal extension
ü Extension to rectum and bladder
ü Ganglionic extension
Imaging strategy to evaluate cervical cancer
• MRIèall patients with a proven cancer (except FIGO IV)
Including thin T2 slices perpendicular to the cervix + sequences exploring the urinary tractus and the para-aortic gangliona
• Contrast-enhanced computed tomography as an alternative to MRI if this latter is not feasable
Should be thoraco-abdomino pelvic for all FIGO IV
• PET Scanner if no surgery is scheduled
Cystoscophy + rectosigmoidoscopy if corresponding lesions can not be eliminated
For these reasons,
MRI offers the opportunity to accurately characterize the extension of the cervical cancer
Accuracy= 80-96% (vs.
70% for the clinical stadification)
INFORMATIONS TO INCLUDE IN THE REPORT
qTumor size.
qUterus
qParametrial extension.
qUreters.
qBladder and rectum
qGanglia.
qMetastasis.
TECHNICAL CONSIDERATIONS
Mid bladder repletion
Sober (4-6h)
Reduce peristaltic motion (IV ou IM,
1mg Glucagon) before the exam
Abdominal contention to limit respiratory artefacts
- Intra- vaginal ultra sound gel
RADIOANATOMY
Cervix
- T1 sequence : homogenous,
iso-intense to pelvic muscles
- T2 sequence :
-
- target sign with 3 concentric layers
- T1 gadolinum enhanced sequence: central hypervascular zone corresponding to the cervical mucosa
Parametrium
- Fibrous and fatty connective tissue that surrounds the uterus
- Limits= cervix + 2/3 of the vagina
- In T2 ponderation : hypersignal / stroma
- Intense enhancement after Gadolinium injection
MRI PROTOCOLE
ü Fast for 4 h before examination to reduce small bowel peristalsis artifacts.
ü Axial T1W : 256 × 256 matrix,
32 cm field of view (FOV),
4 mm slice thickness,
1 mm interslice gap
ü High-resolution T2W images of pelvis are acquired in axial,
sagittal,
and coronal planes using 512 × 256 matrix,
24 cm FOV,
4 mm slice thickness,
1 mm interslice gap for the evaluation of primary tumor spread.
It allows the evaluation of tumor extension to the body of uterus,
vagina,
parametrium,
rectal wall,
and urinary bladder wall.
ü Oblique axial T2W images planned perpendicular to the long axis of cervix give more accurate assessment of stromal involvement and parametrial invasion.
ü Fat-suppressed sequences can be useful for the evaluation of parametrial involvement.
ü Post-contrast images are obtained in axial,
coronal,
and sagittal planes,
and are useful to identify bladder and rectal wall invasion,
fistulas,
and in the detection of recurrent tumor.
Dynamic images obtained 30-60 seconds after gadolinium injection are helpful for the assessment of smaller tumors which are not visible on T2W images as they show increased early contrast enhancement relative to the cervical stroma
TUMOR CHARACTERISTICS
T2: Moderate hypersignal contrasting with the hyposignal of the fibrotic cervical stroma
T1: isosignal compared to the cervix (usually not visible)
Dynamic sequences= early enhancement of tumors with small size compared to a normal cerix
VAGINAL EXTENSION
MRI semiology:
Localized interruption of the T2 hyposignal of the vaginal wall +/- parietal thickening with a T2 hyperintense signal
-IIA: involvement up to the upper 2/3 of the vagina
-IIIA: involvement of the lower 1/3 of the vagina
Anatomical landmarks:
ü Upper 1/3 = culs de sac vaginaux
ü Mid 1/3 = vesical
ü Inferior 1/3 = reste du vagin
MRI performance
ü Diagnostic accuracy in litterature= 83-100%
ü optimisation by the use of intravaginal gel
Causes of diagnostic errors
ü False positive of vaginal involvment in the presence of a voluminous exophytic tumors retracting the vaginal pouch
ü False negative in the presence of microscopic lesions
PARAMETRIAL EXTENSION
MRI semiology:
Complete interruption of the fibrotic stromal annulus of the cervix associated to a tumoral lesion or to a signal of parametrial involvment
Parametrial extension= IIB
MRI performance
ü Diagnostic accuracy= 88%
ü To improve the diagnostic accuracy: usually perform a T sequence with axial sections perpendicular to the cervix èthis allows a circumfrential analysis of the fibrotic stromal annulus
ü Essential message= MRI reliably identifies candidates to surgeryèit accurately eliminates a parametrial involvement (high negative predictive value)
Causes of diagnostic errors
ü False negatives: in case of microscopic tumor foci
ü False positives: The "isolated" interruption of the cervical fibrous stromal ring signifies the invasion of the whole thickness of the stroma and does not necessarily mean the achievement of the parameter opposite
- - In literature: associated with parametrial invasion in 30 to 73% of cases
- Look for other evocative MRI signs:
-
- irregular tumor-parameter interface
- cranial-caudal tumor diameter> 3 cm
- linear spicules in peritumoral parametral fat
- engulfment of peri-uterine vessels
- False positives:
-
- "Pseudo-interruption" of the fibrous cervical stroma,
which is actually very thin in case of voluminous lesion enlarging the cervical canal
- In case of exophytic cervical lesion developed towards the vagina,
the interruption of the fibrous stromal ring does not translate a parametrial invasion when the tumor remains surrounded by a wall of the vaginal pouch uninjured.
-
LYMPH NODE EXTENSION
- Lymph node status determines the choice of adjuvant therapy (radiotherapy)
- Diagnostic features in MRI:
- small axis > 10 mm
- T2 intermediate signal
- Shape : rounded more suspicious than oval
- Contours: lobulated or spiculated contours more suspect than smooth contours
- Enhancement: annular enhancement with central necrosis = predictive of metastases (VPP = 100% according to AJR 2000,
Yang et al)

 and coronal (b) sections
Cervical lesion extending to anterior vaginal wall and to the left parametria as attested by the loss of the pericervical hypo-intense signal
IIB proximal")
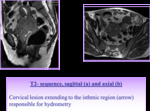
, axial (b)
Left iliac lymphadenopathy measuring 1 0 mm.")