ECR 2019 / C-3680
Preoperative imaging of malignant pancreatic tumors: a key determinant in assessing the resecability
Congress:
ECR 2019
Poster Number:
C-3680
Type:
Scientific Exhibit
Keywords:
Neoplasia, Metastases, Cancer, Diagnostic procedure, Contrast agent-intravenous, MR, CT, Pancreas, Oncology, Abdomen
Authors:
G. Berrada, K. Charef, Z. Abbad El Andaloussi, H. El Mrabet, H. LHAJOUI, S. El Manjra, S. lezar, M. P. F. Essodegui, K. Elkhadir; Casablanca/MA
DOI:
10.26044/ecr2019/C-3680
:343-357")
Fig. 1
. References: Agostini S. Radioanatomie du pancréas. EMC (Elsevier Masson SAS, Paris), Radiologie et imagerie médicale - abdominale - digestive, 33-650-A-10, 2010")
Fig. 2:
I. Head
II. Neck
III. Body
IV. Tail
The uncinate process is behind...
 Abutment of the C with the V; (B) encasement; and (C) involvement/invasion with teardrop deformity. C:cancer; V:vessel References: Imaging preoperatively for pancreatic adenocarcinoma, Jason Alan Pietryga et al, J Gastrointest Oncol 2015;6(4):343-357")
Fig. 3:
Cartoon depiction of vascular involvement. (A) Abutment of the C with the V;...
 without lymphadenopathy or metastatic disease. C:disease extending beyond the pancreas without vascular involvement (T3),lymphadenopathy, or metastatic disease. E:disease with lymphadenopathy. D: disease with vascular involvement (T4). F:disease with distant metastatic disease. Blue = superior mesenteric vein, red = superior mesenteric artery, brown = tumor, gold = lymphadenopathies and liver metastases, light blue = inferior vena cava, pink = aorta. References: Pancreatic adenocarcinoma staging in the era of Preoperative Chemotherapy and Radiation therapy, Marc Zins et al, Radiology 2018; 287:374–390")
Fig. 4:
Staging of pancreatic adenocarcinoma: A, B:disease with the primary tumor...
 with a high enhancement in the pancreatic phase: it was an insulinoma in a 32 year-old women revealed by hypoglycemia. No metastatic disease was detected.It was staged T1N0M0.")
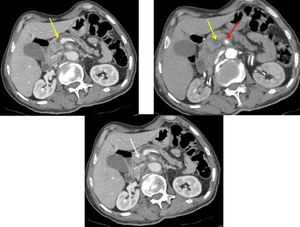
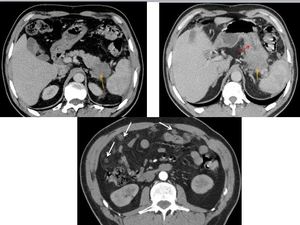
Fig. 5:
A small resecable pancreatic tumor detected in the neck of the pancreas (yellow...
 with dilatation of pancreatic, intrahepatic and extrahepatic ducts (red arrows). The tumor is staged T2 > 4cm, without vascular involvment of SMA (white arrow) and SMV (blue arrow). There is a nodal involvment (N1) and no liver metastasis (M0).")
Fig. 6:
A resecable pancreatic adenocarcinoma in a 56 year-old-women involving the head...
 withour dilatation of downstream ducts because head was not involved. Diffusion images were caracteristic and revealed the tumor with a low ADC (yellow arrows). No vascular involvment was found.")
Fig. 7:
A resecable pancreatic ductal adenocarcinoma in the uncinate process of the...
 in a 58 years old man. It was staged: T1<4cm, N0: no nodal involvment, M0: no metastatic lesions. No vascular involvment was found.")
Fig. 8:
A pancreatic resecable adenocarcinoma of the uncinate process (orange arrow) in...
 in a 63-year-old women. CT revealed a dilatation of both upstream and downstream pancreatic ducts (yellow arrows), an abutment of SMV (blue arrow)without contact with SMA.")
Fig. 9:
A bordeline resecable pancreatic ductal adenocarcinoma of the head of the...
, a narrowing of SMV (yellow arrow), with collateral circulation (blue arrow). Red arrow: no contact with SMA.")
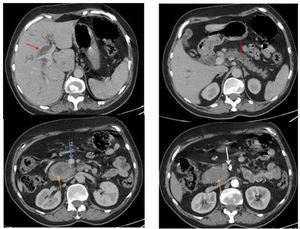
Fig. 10:
A bordeline resecable pancreatic ductal adenocarcinoma involving the head in...
 with both dilatation of pancreatic ducts upstream and downstream the tumor (yellow arrows) and hepatic metastatic (red arrow). It was staged T2N1M1.")
Fig. 11:
An unresecable pancreatic ducatl adenocarcinoma in a 70-year-old man presenting...
 with only peripheral enhancement. There are metastatic hepatic lesions revealed on diffusion imaging (red arrows).")
Fig. 12:
An unresecable pancreatic ductal adenocarcinoma of the tail of the pancreas in...
 in a 66 year-old-man with invasion of the superior mesenteric vein (blue arrow) and liver metastasis (M1): red arrows.")
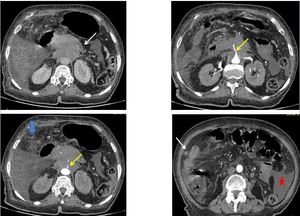
Fig. 13:
CT images shows an unresecable pancreatic adenocarcinoma of the uncinate...
, vascular involvement :narrowing of celiac axis and SMA (yellow arrows). There is also a metastatic peritoneal thickening (blue arrow) and ascites (red star)")
Fig. 14:
An unresecable pancreatic ductal adenocarcinoma in a 78-year-old women...
 in a 62 years old man with involvment of the stomach (red arrow). There are many peritoneal nodules (a distant metastatic disease). It was staged T3N1M1.")
Fig. 15:
An unresecable tail pancreatic adenocarcinoma (orange arrows) in a 62 years old...
 with dilatation of upstream pancreatic duct (yellow arrows) and narrowing of SMA (red arrow).")
Fig. 16:
An unresecable pancreatic ductal adenocarcinoma of the neck and the body of the...

Fig. 18:
Criteria Defining Resectability Status of Pancreatic Ductal Adenocarcinoma. PV...

Fig. 19:
CT Findings in Visually Isoattenuating Pancreatic Adenocarcinoma Patients