ECR 2019 / C-3724
CT scan evaluation of peritoneal carcinomatosis and its spread patterns according to primary tumors
Congress:
ECR 2019
Poster Number:
C-3724
Type:
Educational Exhibit
Keywords:
Metastases, Education and training, Cancer, Structured reporting, Localisation, Diagnostic procedure, PET-CT, MR, CT, Peritoneum, Mesentery, Abdomen
Authors:
M. Kamoun1, D. D. Muntean2, D. S. Feier2; 1Cluj/RO, 2Cluj-Napoca/RO
DOI:
10.26044/ecr2019/C-3724

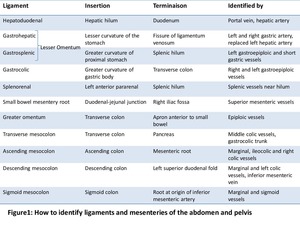
Fig. 1

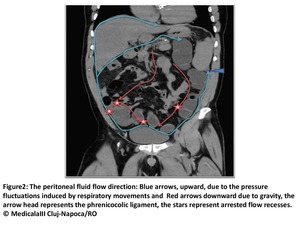
Fig. 2

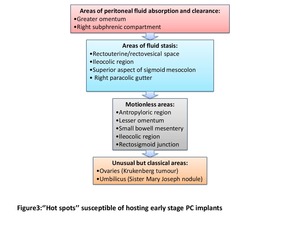
Fig. 3

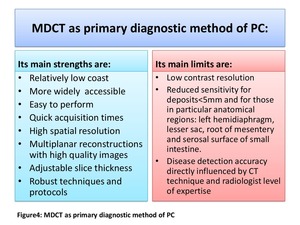
Fig. 4

Fig. 5

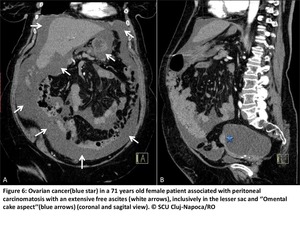
Fig. 6

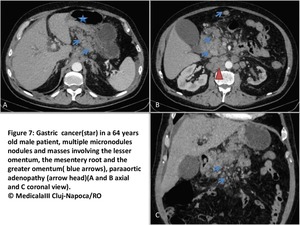
Fig. 7

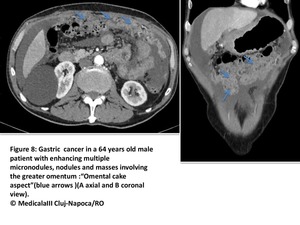
Fig. 8

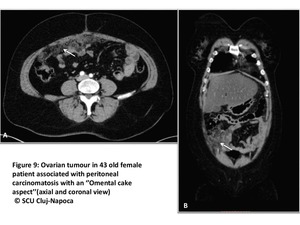
Fig. 9

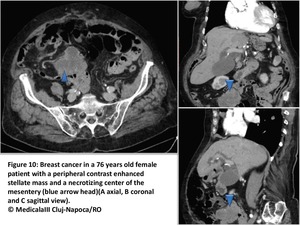
Fig. 10

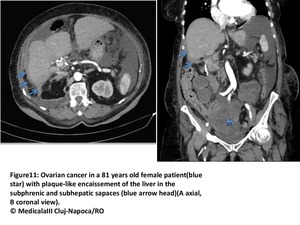
Fig. 11

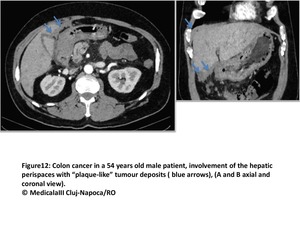
Fig. 12

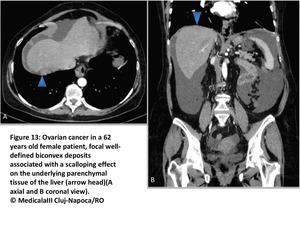
Fig. 13

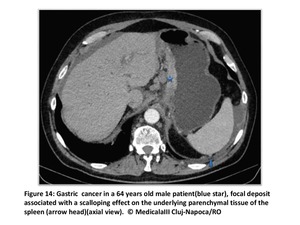
Fig. 14

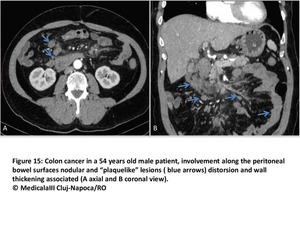
Fig. 15

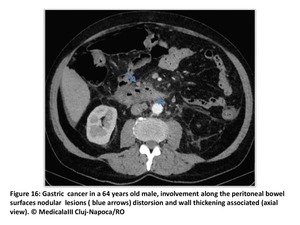
Fig. 16

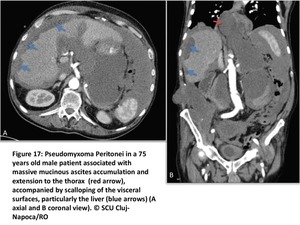
Fig. 17

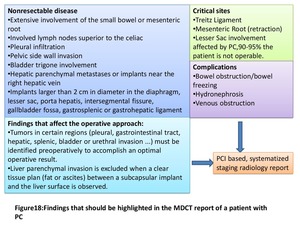
Fig. 18

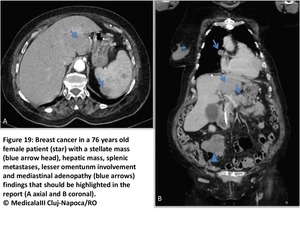
Fig. 19

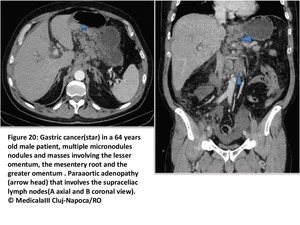
Fig. 20

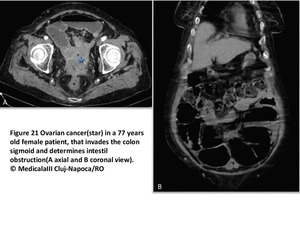
Fig. 21

Fig. 22

Fig. 23

Fig. 24

Fig. 25

Fig. 26

Fig. 27

Fig. 28

Fig. 29

Fig. 30

Fig. 31

Fig. 32

Fig. 33

Fig. 34

Fig. 35

Fig. 36