ECHINOCOCCOSIS
Mainly caused by E. granulosus.
Definitive host are dogs and intermediate hosts are usually sheep or goats.Humans accidentally become intermediate hosts after ingestion of worm's eggs(2)
Type I cyst(WHO CL,WHO CE1) - unilocular, presence of denser material in cyst (falling snowflakes inside cyst in US, or higher attenuation contents in CT), and low signal intensity rim in T2WI MR (11,12).
Type II cysts (WHO CE 2) contain daughter cysts in periphery appearing as multiseptated cysts. Mother cyst has denser content than daughter cysts and appear as higher attenuation in CT and with different signal intensity in MR (13,14). Contained ruptures of the cyst due to trauma etc appear as floating membranes (water-lily sign) and are classified as WHO CE 3 (12, 15). WHO stage CE 4 is between type II and type III cysts.
Type III cyst (WHO CE 5) - chronic ,almost completely calcified. Calcifications are typically curvilinear. (11, 12, 16).
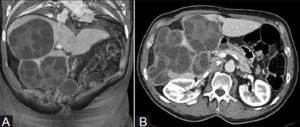
Fig. 1: A case of hydatid cyst .Preprocedure volume rendered CT scan reconstructions show multiple multivesiculated, honeycomb-like, hydatid cysts (type CE2) at the level of the VIII-VII and IV liver segments (A) and within the V-VI liver segments.
References: Corona, Mario, et al. "Case report: Percutaneous treatment of multiple honeycomb-like liver hydatid cysts (type III CE2, according to WHO classification)." The Indian journal of radiology & imaging 22.1 (2012): 23.
SCHISTOSOMIASIS
Most of the imaging findings are due to chronic hepatic affection and its related complications. US display periportal fibrosis as echogenic cuffing and other findings like irregular liver surface, heterogeneous parenchyma etc
CT - findings of chronic hepatopathy and portal hypertension. Periportal fibrosis appears as hypoattenuating bands around portal branches which enhance after contrast infusion.
MR - chronic hepatic schistosomiasis shows periportal cuffing with high signal on T2WI and iso to hypointense on T1WI(2)
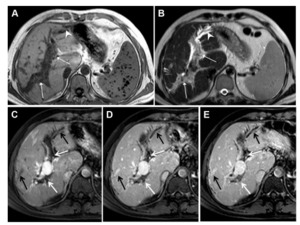
Fig. 8: A case of schistosomiasis - T1-W and T2-W axial MR images demonstrate widened periportal spaces elongated toward the subcapsular location at the periphery. These periportal spaces on the T1-weighted image (A) reveal a hypointense signal characteristic and, on the T2-W image (B), a hyperintense signal characteristic which reflects periportal inflammatory edema due to schistosomiasis (arrows). Signal void spaces due to siderotic nodules are seen in the spleen. Dilated bile ducts are more discernible on the T2-weighted image (arrow heads). Dynamic contrast-enhanced T1-weighted fat-saturated scans at arterial phase (C), portal venous phase (D), and late venous phase (E): As time goes on, contrast enhancement increases in widened periportal spaces (white arrows). Bile duct dilatations and increased contrast enhancement on thickened bile duct walls (black arrows) compatible with cholangitis are also present.
References: Bilgin SS, Toprak H, Seker M. Imaging findings of hepatosplenic schistosomiasis: a case report. Radiology case reports. 2016 Sep 1;11(3):152-6.
ASCARIASIS
Barium fluoroscopy and US play major role in diagnosis.
Barium examination - adult worms in bowel appear as tubular smooth radiolucent filling defects.
US - long echogenic filling defects without acoustic shadowing inside intestinal lumen
MR - T2 hypointense and T1 iso to hypointense cylindrical filling defects .MR cholagiopancreatographic sequences display worms as hypointense tubular structures (17).
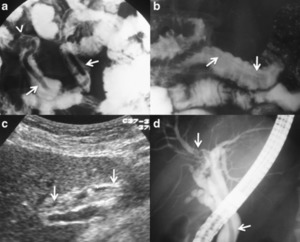
Fig. 4: Ascariasis. a. Barium fluoroscopic study of a 24-year-old woman previous history of ascariasis. The study shows a worm inside a jejunal loop (arrows). The faeces examination revealed ascaris eggs. Note that the head (blunt) of the worm points proximally (arrowhead), as is usual in this parasite b. Barium fluoroscopic study of a 37-year old male shows intestinal worms compatible with ascaris, note that the shown worm has swallowed barium contrast (arrows). c and d. 29-year-old woman with previous surgery of cholecystectomy. The US examination in C displayed a long echogenic filling defect without acoustic shadowing inside the common bile duct (CBD) (arrows), with other adjacent smaller filling defects compatible with gallstones and/or debris. The ERCP in D shows a worm inside the common bile duct whose head is introduced in the right hepatic duct (arrows).
References: - Carnero PR, Mateo PH, Martín-Garre S, Pérez ÁG, Del Campo L. Unexpected hosts: imaging parasitic diseases. Insights into imaging. 2017 Feb 1;8(1):101-25.
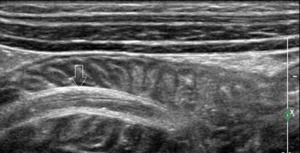
Fig. 5: A case of ascariasis.Ultrasonographic image of abdomen with high frequency transducer showing hypoechoic linear tubular structures with echogenic outer walls and central canals of the worms seen in the lumen of the small intestine (open white arrow).
References: Suthar PP, Doshi RP, Mehta C, Vadera KP. Incidental detection of ascariasis worms on USG in a protein energy malnourished (PEM) child with abdominal pain. Case Reports. 2015 Mar 12;2015:bcr2014206668.
STRONGYLOIDIASIS
Strongyloides stercolaris inhabits small bowel of humans. Larvae penetrate the skin and reach lungs.
During phase of autoinfection, chest radiographs or CT show fine miliary nodules or reticular interstitial opacities.
In heavier infection - bronchopneumonia with patchy alveolar opacities, segmental opacities and lobar migratory opacities may be present (18, 19).
In hyperinfection syndrome - extensive pneumonia, pulmonary haemorrhage, and pleural effusion.(2)
DRACUNCULIASIS
It is a subcutaneous disease caused by Dracunculus medinensis and is transmitted to humans through drinking water contaminated with Cyclops. Dead calcified worms can be seen incidentally as soft tissue worm-like calcifications on radiographs or CT.(2)

Fig. 2: Dracunculiasis. a and b Plain radiographs of the left knee and leg of a patient shows “worm-like” calcifications in the soft tissues caused by dead calcified worms. c. CT image of the left leg of the same patient as in a and b, confirms the dead calcified worms in the subcutaneous tissue and muscles of the left lower limb
References: Carnero PR, Mateo PH, Martín-Garre S, Pérez ÁG, Del Campo L. Unexpected hosts: imaging parasitic diseases. Insights into imaging. 2017 Feb 1;8(1):101-25.
CYSTICERCOSIS
Cysticercosis is caused by Taenia solium. Their definitive hosts are humans and intermediate hosts are pigs.Neurocysticercosis is classified in five stages regarding their evolution from active larvae to dead lesions as non-cystic, vesicular, colloidal vesicular, granular nodular, and calcified nodular.(20,21)
The vesicular stage - cyst or group of cysts (racemose form) containing the larvae. The cyst has content similar to CSF in CT and MR and protoscolex can be seen as eccentric dot with high signal intensity on T1WI, the ‘cyst with dot sign’. No surrounding oedema and enhancement is seen ( 20, 22-24).
Colloidal vesicular stage - parasite begins to degenerate and host develops a stronger immune response. The fluid of cyst appears as higher signal on MR and higher attenuation on CT. The inflammatory response leads to surrounding oedema and ring enhancement of the cyst (22, 25).
Granular nodular phase -cyst shrinks, acute immune response decreases, and is progressively replaced by gliosis, imaging findings are similar to colloidal vesicular stage.
Calcified nodular phase - represents dead parasite. CT is superior to MR when detecting the calcified lesions of this stage (22).
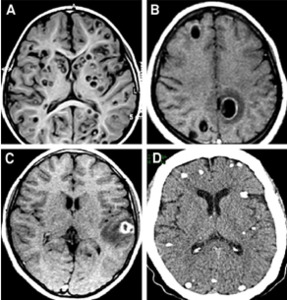
Fig. 3: MRI and CT-scan of parenchymal cysticerci.MRI of vesicular cysticerci (A).MRI of colloidal cysticerci (B).Single hyperintense lesion on MRI (C).CT-scan of calcified cysticerci (D).
References: Carpio, Arturo, and Matthew L. Romo. "The relationship between neurocysticercosis and epilepsy: an endless debate." Arquivos de neuro-psiquiatria 72.5 (2014): 383-390.
TRICHURIASIS
Trichuris eggs are transmitted through fecal-oral route. After their elimination in feces, Trichuris eggs become infective within 15 to 30 days. Upon ingestion, the eggs release larvae in small intestine. The larvae mature during their migration to the cecum and ascending colon, where the adult worms attach themselves to mucosa. Barium enema examination depict worms as small elongated filling defects.(3)
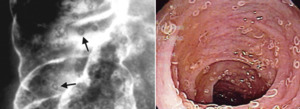
Fig. 6: A case of trichuriasis .Image from a barium enema examination in a 4-year-old patient with rectal bleeding and anemia shows mucosal thickening and multiple tiny filling defects with a curvilinear shape (arrows). (b) Image from colonoscopy shows multiple T trichiura worms attached to the cecum.
References: Ortega CD, Ogawa NY, Rocha MS, Blasbalg R, Caiado AH, Warmbrand G, Cerri GG. Helminthic diseases in the abdomen: an epidemiologic and radiologic overview. Radiographics. 2010 Jan;30(1):253-67.


 at the level of the VIII-VII and IV liver segments (A) and within the V-VI liver segments. References: Corona, Mario, et al. "Case report: Percutaneous treatment of multiple honeycomb-like liver hydatid cysts (type III CE2, according to WHO classification)." The Indian journal of radiology & imaging 22.1 (2012): 23.")
 reveal a hypointense signal characteristic and, on the T2-W image (B), a hyperintense signal characteristic which reflects periportal inflammatory edema due to schistosomiasis (arrows). Signal void spaces due to siderotic nodules are seen in the spleen. Dilated bile ducts are more discernible on the T2-weighted image (arrow heads). Dynamic contrast-enhanced T1-weighted fat-saturated scans at arterial phase (C), portal venous phase (D), and late venous phase (E): As time goes on, contrast enhancement increases in widened periportal spaces (white arrows). Bile duct dilatations and increased contrast enhancement on thickened bile duct walls (black arrows) compatible with cholangitis are also present. References: Bilgin SS, Toprak H, Seker M. Imaging findings of hepatosplenic schistosomiasis: a case report. Radiology case reports. 2016 Sep 1;11(3):152-6.")
. The faeces examination revealed ascaris eggs. Note that the head (blunt) of the worm points proximally (arrowhead), as is usual in this parasite b. Barium fluoroscopic study of a 37-year old male shows intestinal worms compatible with ascaris, note that the shown worm has swallowed barium contrast (arrows). c and d. 29-year-old woman with previous surgery of cholecystectomy. The US examination in C displayed a long echogenic filling defect without acoustic shadowing inside the common bile duct (CBD) (arrows), with other adjacent smaller filling defects compatible with gallstones and/or debris. The ERCP in D shows a worm inside the common bile duct whose head is introduced in the right hepatic duct (arrows). References: - Carnero PR, Mateo PH, Martín-Garre S, Pérez ÁG, Del Campo L. Unexpected hosts: imaging parasitic diseases. Insights into imaging. 2017 Feb 1;8(1):101-25.")
. References: Suthar PP, Doshi RP, Mehta C, Vadera KP. Incidental detection of ascariasis worms on USG in a protein energy malnourished (PEM) child with abdominal pain. Case Reports. 2015 Mar 12;2015:bcr2014206668.")
 Axial CT images depict multiple ill-defined non-specific hypoattenuating lesions in the liver parenchyma (arrowheads in a) with small-bowel wall thickening (arrows in b). An enterectomy was performed. (c) Photomicrograph (original magnification, ×40; hematoxylin-eosin stain) of a histologic slice shows the parasite inside a mesenteric arteriole (arrow) with surrounding eosinophilic inflammatory infiltrate. (microscopic image - courtesy of Thales de Brito, MD, PhD, and Fernando Aguiar, MD, Departamento de Patologia da Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil.) References: Ortega CD, Ogawa NY, Rocha MS, Blasbalg R, Caiado AH, Warmbrand G, Cerri GG. Helminthic diseases in the abdomen: an epidemiologic and radiologic overview. Radiographics. 2010 Jan;30(1):253-67.")
:101-25.")
.MRI of colloidal cysticerci (B).Single hyperintense lesion on MRI (C).CT-scan of calcified cysticerci (D). References: Carpio, Arturo, and Matthew L. Romo. "The relationship between neurocysticercosis and epilepsy: an endless debate." Arquivos de neuro-psiquiatria 72.5 (2014): 383-390.")
. (b) Image from colonoscopy shows multiple T trichiura worms attached to the cecum. References: Ortega CD, Ogawa NY, Rocha MS, Blasbalg R, Caiado AH, Warmbrand G, Cerri GG. Helminthic diseases in the abdomen: an epidemiologic and radiologic overview. Radiographics. 2010 Jan;30(1):253-67.")
:253-67.")