ECR 2020 / C-01692

MDCT angiography of the postoperative aorta
Congress:
ECR 2020
Poster Number:
C-01692
Type:
Educational Exhibit
Keywords:
Multicentre study, Diagnostic or prognostic study, Not applicable, Grafts, Dissection, Aneurysms, Technical aspects, Surgery, Diagnostic procedure, CT-Angiography, CT, Cardiovascular system, Arteries / Aorta, Vascular
Authors:
M. Finazzo, C. Duranti, G. Filippone, F. Finazzo, G. Peritore, D. Messana; Palermo/IT
DOI:
10.26044/ecr2020/C-01692

Fig. 16:
Patient with replacement of ascending aorta. Graft has no distinctive imaging...

Fig. 17:
Same patient. Graft is slightly hyperattenuanting on unenhanced CT .

Fig. 18:
Patient with a modified Cabrol procedure. CTA - VRT reconstruction shows small...
 and felt pledgets (yellow arrows), are hyperdense on CT and may mimic contrast material. Unenhanced CT images help differentiate high attenuating surgical material from contrast extravasation")
Fig. 19:
Surgical material, such as felt strips (orange arrows) and felt pledgets...
 and felt pledgets (yellow arrows), are hyperdense on CT and may mimic contrast material. Unenhanced CT images help differentiate high attenuating surgical material from contrast extravasation")
Fig. 20:
Surgical material, such as felt strips (orange arrows) and felt pledgets...
 and felt pledgets (yellow arrows), are hyperdense on CT and may mimic contrast material. Unenhanced CT images help differentiate high attenuating surgical material from contrast extravasation")
Fig. 21:
Surgical material, such as felt strips (orange arrows) and felt pledgets...
 and felt pledgets (yellow arrows), are hyperdense on CT and may mimic contrast material. Unenhanced CT images help differentiate high attenuating surgical material from contrast extravasation .")
Fig. 22:
Surgical material, such as felt strips (orange arrows) and felt pledgets...

Fig. 23:
CTA shows a small outpouching, bulging from the anterior graft wall. This bulge...

Fig. 24:
CTA shows a small outpouching, bulging from the anterior graft wall. This bulge...
, free floating in the descending aorta, can simulate an aortic dissection. However, careful review of CT images on axial, sagittal, coronal and oblique planes and awareness of patient case history can avoid this imaging pitfall.")
Fig. 25:
The graft of the elephant trunk (orange arrows), free floating in the...
, free floating in the descending aorta, can simulate an aortic dissection. However, careful review of CT images on axial, sagittal, coronal and oblique planes and awareness of patient case history can avoid this imaging pitfall.")
Fig. 26:
The graft of the elephant trunk (orange arrows), free floating in the...
, free floating in the descending aorta, can simulate an aortic dissection. However, careful review of CT images on axial, sagittal, coronal and oblique planes and awareness of patient case history can avoid this imaging pitfall.")
Fig. 27:
The graft of the elephant trunk (orange arrows), free floating in the...

Fig. 28:
Endograft looks like a hyper-attenuating tubular mesh on Left Anterior Oblique...

Fig. 29:
False lumen is filled up with thrombus, due to the seal and coverage by the...
 and anastomosis of coronary arteries into the graft (Bentall procedure). CTA shows two large pseudoaneurysms (p) at both the coronary arteries anastomosis sites.")
Fig. 30:
Patient with replacement of ascending aorta and aortic valve with an artificial...
.")
Fig. 32:
The same patient underwent new surgical intervention. The old graft of...

Fig. 33:
Open repair of the thoraco-abdominal aorta in an emergency. A: CTA shows...
 of the infrarenal abdominal aorta, common iliac arteries, external iliac arteries. The bypass is patent. Occluded common iliac arteries stents are noticed.")
Fig. 36:
Axillofemoral bypass in a patient with occlusion (orange arrow) of the...

Fig. 37:
Small floating thrombus in the left limb of the endograft.

Fig. 38:
The presence of air in the excluded peri-graft space should raise concern about...

Fig. 39:
There is a thick-walled abscessual fluid collection in the left psoas muscle...

Fig. 40:
Endograft infection. Axial contrast enhanced CT image and coronal VRT image...

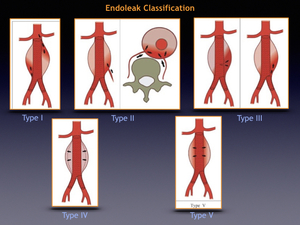
Fig. 41:
Type I endoleak. VRT reconstruction, sagittal and coronal MIP images from CT...

Fig. 42:
Type II endoleak. Sagittal MIP image from CT angiogram show a small collection...

Fig. 43:
Type II endoleak. Coronal MIP image from CT angiogram show a small collection...

Fig. 44:
Type II endoleak. Same patient in figures 55-56. Sagittal MIP image from CT...

Fig. 45:
Type II endoleak. Axial CT from CT angiogram shows a contrast collection within...

Fig. 46:
Type II endoleak. VRT reconstruction from CT angiogram shows a contrast...
.")
Fig. 47:
Breakage of endograft mesh (orange arrow).
.")
Fig. 48:
Sigmoid ischemia in a patient with endograft of the abdominal aorta. Axial...
 in the inferior pole of the spleen.")
Fig. 49:
Splenic infarction. Axial contrast enhanced CT in the same patient in figure 61...

Fig. 50