ECR 2020 / C-02557

Endovascular management of obstetric & gynaecologic conditions: a case-based pictorial review for radiology trainees.
Congress:
ECR 2020
Poster Number:
C-02557
Type:
Educational Exhibit
Keywords:
Not applicable, Haemorrhage, Embolisation, Balloon occlusion, Catheter arteriography, Oncology, Obstetrics (Pregnancy / birth / postnatal period), Interventional Radiology
Authors:
S. Teoh, B. Young; Sarawak/MY
DOI:
10.26044/ecr2020/C-02557
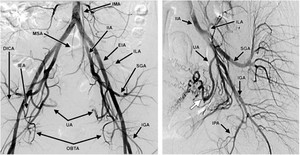
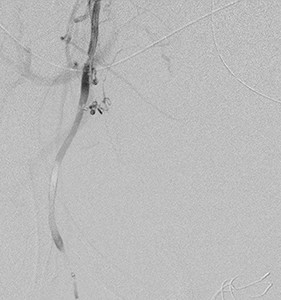
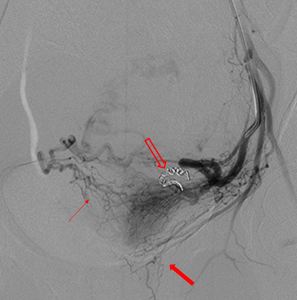
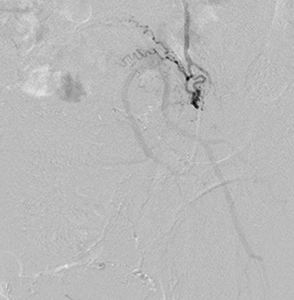
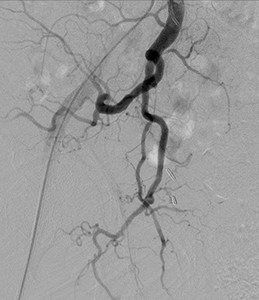
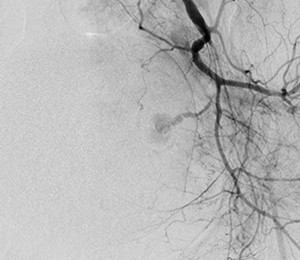
. Digital substraction angiography (DSA) of the pelvic aorta and the magnified left IIA DSA. DCIA= deep iliac circumflex artery, EIA=external iliac artery, IGA=inferior gluteal artery, ILA=iliolumbar artery, IMA=inferior mesenteric artery, IPA=internal pudendal artery, MSA=median sacral artery, SGA=superior gluteal artery, UA=uterine artery, IIA=internal iliac artery, IEA=inferior epigastric artery. References: Katz MD et al. (2012) Beyond hemostasis: Spectrum of gynecologic and obstetric indications for transcatheter embolization. Radiographics. 2012;32(6):1713-1731.")
Fig. 1:
Pelvic iliac artery anatomy. Adopted from reference(2). Digital substraction...
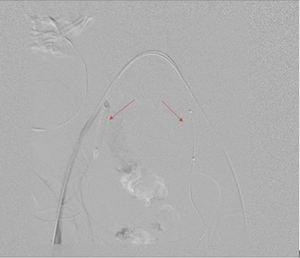
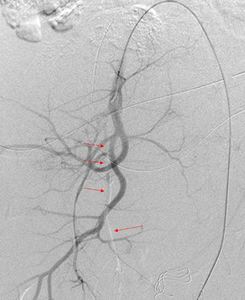
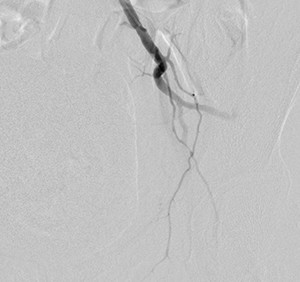
 during test inflation showing no flow to the internal iliac arteries. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 2:
Inflated PTA balloons (arrows) during test inflation showing no flow to the...
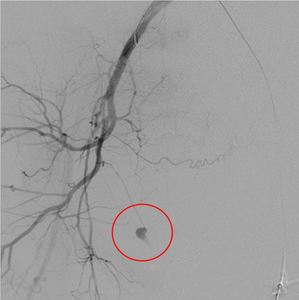
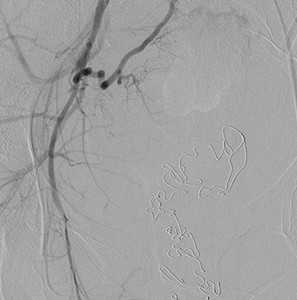
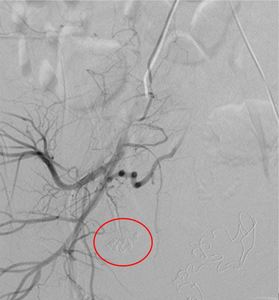
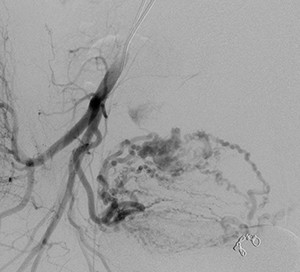
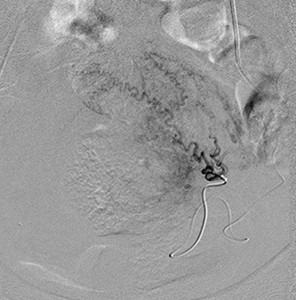
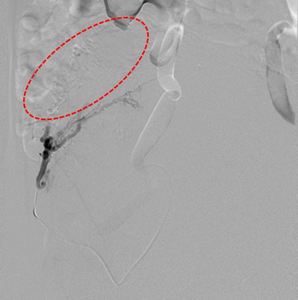
 from a tiny side branch of the right internal pudendal artery. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 3:
Right IIA run showing active contrast extravasation (red circle) from a tiny...

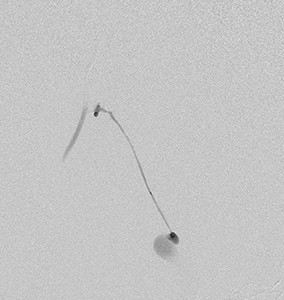
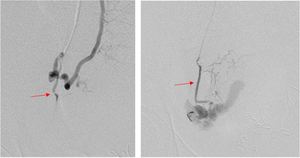
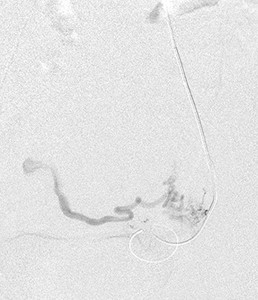
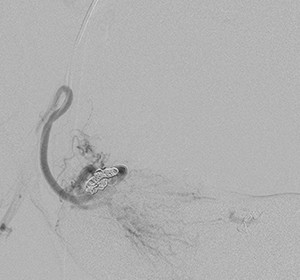
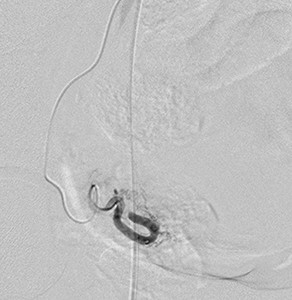
Fig. 4:
Superselective cannulation of the tiny side branch of the internal pudendal...

Fig. 5:
Post embolization with glue emulsion. Run showed complete occlusion of the side...
. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 6:
Post gelfoam embolization of the anterior division of the right IIA for further...

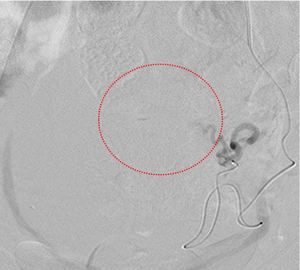
Fig. 7:
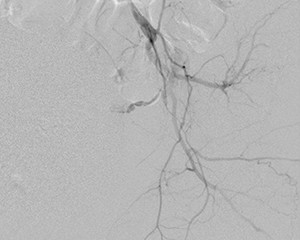
Initial right IIA run showing no obvious contrast extravasation or blush.
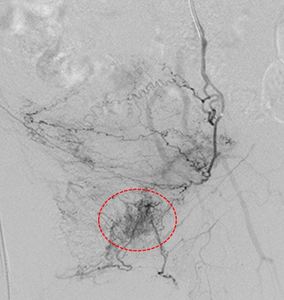
 which confirmed active bleeding (red arrow) on further ultraselective cannulation of this branch. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 8:
Subsequent cannulation of right uterine artery unveiled a tiny suspicious...

Fig. 9:
Post embolization with Glue-lipiodol emulsion in acquired image
 branching from the right uterine artery. Bilateral anterior trunk of internal iliac arteries bilaterally embolised prophylactically as well (images not shown). References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 10:
Post embolization run show complete occlusion of the right vaginal artery (red...
. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
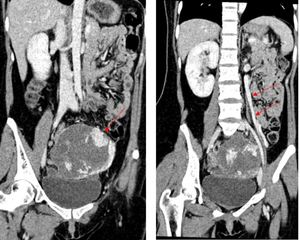
Fig. 11:
Plain CT abdomen in coronal view show a heterogenous pelvic mass with fetal...
 locating outside of the uterus, superior to the uterine fundus and urinary bladder. The abnormal vasculature within may be part of the placental tissues (red arrows). References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 12:
CT angiogram of the abdomen in sagittal view showing the distinct pelvic mass...
 draining from the fetal pelvic mass suggestive of either an ovarian origin or arteriovenous fistula within the fetal/placental tissue. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 13:
Portovenous phase of CT Abdomen in coronal view showing an abnormally dilated...

Fig. 15:
Selective cannulation of the left uterine artery as distal as possible to avoid...
 run showed occlusion of the left uterine artery with opening of the inter-uterine collaterals (thin red arrow) supplying the ectopic pregnancy. The normal supply to the uterus is preserved, vaginal branches are visualized now and preserved (broad red arrow). References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 16:
Post embolization with platinum coil (hollow broad red arrow) run showed...

Fig. 17:
Right IIA run showing the other part of the ectopic pregnancy’s abnormal...

Fig. 18:
Post embolization with platinum coil run show occlusion of the uterine supply...

Fig. 20:
Superselective cannulation of the smaller distal branches supplying the tumour...
. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 21:
Post embolization with PVA particles run showing reduction in tumoural blush...
 with supply from a dilated tortuous right uterine artery. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 22:
Right IIA run showing a large tumoural blush (red dotted circle) with supply...

Fig. 23:
Post superselective cannulation of smaller supplying uterine branches to the...
 with tiny supplying vessels from the presumably cervicovaginal branches. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 24:
Left IIA run showing small tumoural blush (red circle) with tiny supplying...
. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 25:
Superselective cannulation of the tiny cerviovaginal branches with better...

Fig. 26:
Post embolization with PVA particles and gelfoam emulsion run showing complete...

Fig. 27:
No demonstrable tumoural blush from the right IIA.
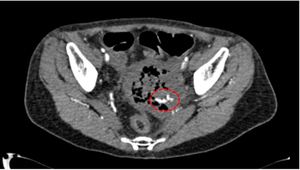
 and axial view (Fig 28) showing contrast blush (red circle) within the vaginal packing adjacent to the cervical mass which persist with dispersal on delayed 3 minutes (not shown) indicative of active haemorrhage. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 28:
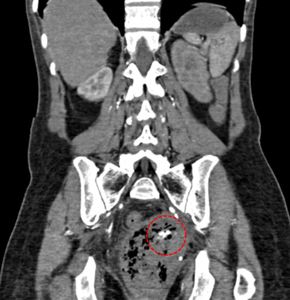
CT angiogram of the abdomen in coronal (Fig 29) and axial view (Fig 28) showing...
 and axial view (Fig 28) showing contrast blush (red circle) within the vaginal packing adjacent to the cervical mass which is persistent with slight dispersal at delayed 3 minutes scan(not shown) indicative of active haemorrhage. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 29:
CT angiogram of the abdomen in coronal (Fig 29) and axial view (Fig 28) showing...

Fig. 30:
Left IIA run showing focal contrast blush corresponding to the findings on CT...

Fig. 31:
Superselective cannulation of the tiny branch attributing to the contrast...

Fig. 32:
Post embolization with gelfoam showing resolution of the contrast...
 at the right lower abdomen. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 33:
Flush pelvic aortogram showing large fibroid blush (red circle) at the right...
 supplying the large fibroid. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 34:
Anterior division of right IIA run showed ascending uterine arterial branches...
. References: Department of Radiology, Sarawak General Hospital – Sarawak/MY")
Fig. 35:
Superselective cannulation of the ascending uterine arterial supply with post...