ECR 2020 / C-14516
Angiosarcoma of the breast, a forgotten tumor
Congress:
ECR 2020
Poster Number:
C-14516
Type:
Educational Exhibit
Keywords:
Breast, Oncology, Mammography, MR, Ultrasound, Contrast agent-intravenous, Cancer, Not applicable
Authors:
D. SÁNCHEZ GARCIA, A. Fernández Tamayo, P. ELVIRA RUIZ, J. CABO BOLADO, J. M. Zulueta Odriozola, E. García Laborda, F. J. Olcoz Monreal, O. Bueno Zamora; Madrid/ES
DOI:
10.26044/ecr2020/C-14516
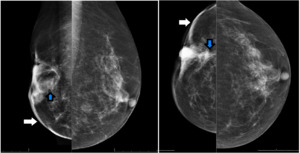
 in lower quadrants and a mass (blue arrows) in the middle of the lower outer and inner quadrants of the right breast with mixed density and ill-defined margins.")
Fig. 1:
55 years old women with right breast cancer treated with radiation therapy +...
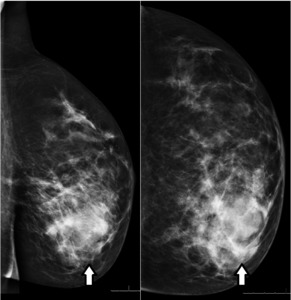
 in the inner lower quadrant with mixed density and ill-defined margins.")
Fig. 2:
48 years old women. MLO and CC of left breast shows a mass (white arrows) in...
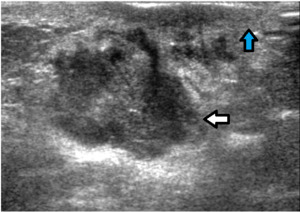
 in the middle of the lower outer and inner quadrants with mixed echogenicity and not-circumscribed margins, without posterior shadowing. The mass contacts the skin (blue arrow), which is thickened.")
Fig. 3:
Same patient in figure 1. Ultrasonography of the right breast demonstrate an...

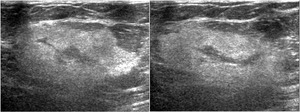
Fig. 4:
Same patient in figure 2. Ultrasonography of the left breast demonstrate an...
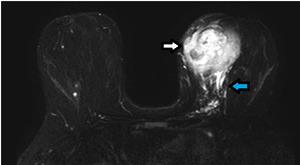
 in the inner lower quadrant with high signal. Posteriorly, tubular structures of high signal intensity (blue arrow) are noted representing large draining vessels.")
Fig. 5:
Same patient in figures 2 and 4. MRI of both breasts,T2/SPAIR sequence. We can...

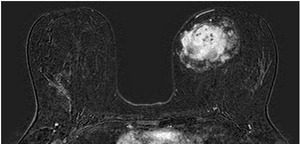
Fig. 6:
Same patient in figures 2, 4 and 5. MRI of both breasts, post-gadolinium T1/FFE...
 in the delayed phase.")
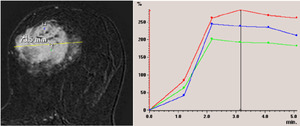
Fig. 7:
Same patient in figures 2, 4, 5 and 6. Kinetic analysis of the mass seen in the...