
ECR 2022 / C-10921

ECR 2022: Building bridges between coronary artery geometry and atherosclerosis - an educational poster enlightening pathophysiology and potentialities in the era of state-of-the-art coronary CTA
Congress:
ECR 2022
Poster Number:
C-10921
Type:
Educational Exhibit
Keywords:
Cardiac, CT-Angiography, Diagnostic procedure, Arteriosclerosis
Authors:
V. Rafailidis, G. Rampidis, K. Kouskouras, A. Davidhi, A. PAPACHRISTODOULOU, G. Giannakoulas, H. Karvounis, P. Prassopoulos
DOI:
10.26044/ecr2022/C-10921
Findings and procedure details

Fig 1:
Table 1. The multi-factorial pathogenesis of atherosclerosis

Fig 2:
Table 2. Findings and definitions used in angiographic study of autopsy hearts.

Fig 3:
Table 3. List of geometric features of coronary arteries

Fig 4:
A triad for coronary atherosclerosis pathogenesis analogous to Virchow triad.

Fig 5:
Assessment of total vulnerability burden for superior cardiovascular risk...
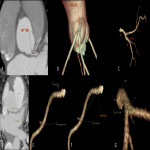
Fig 6:
Examples of coronary geometric features measurements. Angle measurement on MIP...
, an S-shaped (B) RCA and an RCA with focal angulation (C).")
Fig 7:
Examples of a C-shaped (A), an S-shaped (B) RCA and an RCA with focal...

Fig 8:
Table 4. Key associations between coronary geometry and atherosclerosis

Fig 9:
Table 5 Geometric features associated with hemodynamic alterations
, a left circumflex with angulation and peripheral calcification (B) and a bifurcation with proximal plaques (C). A left circumflex artery with tortuosity (D).")
Fig 10:
Examples of left coronary circulation. A bifurcation with proximal disease (A),...
 and a large (B) angle measured on volume rendering images.")
Fig 11:
Examples of left main artery bifurcations with a small (A) and a large (B)...

Fig 12:
Examples of left anterior descending artery with low (A), high (B) tortuosity...

Fig 13:
Quantification of coronary atherosclerosis in the assessment of coronary artery...

Fig 14:
Volume-rendering and multiplanar reconstruction techniques used to measure the...

Fig 15:
Images acquired with CCTA demonstrates vulnerable, non-obstructive,...

Fig 16:
The left bifurcation angle was measured 350 in a 70-year-old man with minimal,...