
ECR 2023 / C-16634

Tips and tricks of Sinonasal Computed Tomography
Congress:
ECR 2023
Poster Number:
C-16634
Type:
Educational Exhibit
Keywords:
Ear / Nose / Throat, Cone beam CT, CT, Complications, Education and training
Authors:
E. Marín Díez, J. Viera-Artiles, M. Arroyo Olmedo, A. Berasategui Criado, S. M. Bretos Azcona, C. Cantolla Nates, M. Barrios López, M. J. Galante Mulki, E. Julián Gómez
DOI:
10.26044/ecr2023/C-16634
Findings and procedure details
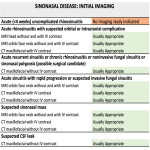
Table 1:
ACR Appropriateness CriteriaSinonasal Disease: 2021 Update. Reference 1.
. Mucosal thickening is demonstrated along the nasal cavity and maxillary sinuses (yellow arrow in A). Note leading edge of dense bone (blue arrow in A) overlying less dense bone (blue asterisk in A). Image B shows saddle nose deformity (yellow arrow).")
Fig 2:
Granulomatosis with polyangiitis. Patient with a history of granulomatosis with...

Fig 3:
CT anatomy of superior and inferior turbinates.
: A-B, CT coronal images of OMC with the different anatomical parts labelled in B. C shows a CBCT coronal image where the left OMC is completely obliterated in a patient with acute sinusitis.")
Fig 4:
CT anatomy of ostiomeatal complex (OMC): A-B, CT coronal images of OMC with the...

Fig 5:
Ostiomeatal complex anatomical variations.

Fig 6:
Anatomy of the middle turbinate. The basal lamella is pointed with the green...

Fig 7:
Ethmoid bone´s anatomy.

Fig 8:
CT anatomy of the olfactory fossa.

Fig 9:
Anterior ethmoid artery.

Fig 10:
Haller and Onodi cells.

Fig 11:
Maxillary sinus.

Fig 12:
Sphenoid sinus.

Fig 13:
Frontal sinus.

Table 2:
Structured reporting. Reference 2.

Fig 1:
Nasal septum. Reference 4 for image C.
. The below images show the frontal sinus air outflow track depending on the presence of a supra Agger frontal cell or a supra bulla frontal cell.")
Fig 14:
Frontal Sinus Anatomy Classification (IFAC). The below images show the frontal...