Anterior impingement syndrome
Anterior ankle impingement is a well established and relatively common cause of chronic ankle pain,
particularly in soccer players,
runners and ballet dancers,
who sustain repetitive ankle dorsiflexion.
Symptoms are generally progressive and relate to impingement of hypertrophied synovial scar tissue and bony spurs within the anterior ankle joint.
Anatomy and pathophysiology
Ankle instability or repetitive forceful dorsiflexion can result in microtrauma to the anterior joint cartilage and deeper bone layers.
Over time,
attempted repair including fibrosis and fibrocartilage proliferation leads to the formation of bony spurs on the anterior rim of the tibia and sulcus of the talus2.
These bony spurs or osteophytes can cause anterior joint space narrowing,
limiting ankle dorsiflexion (Fig. 1)3.
The term osteophyte does not infer imply conventional osteoarthritis,
rather a proliferative effect of focal premature degeneration.
Like any other osteophyte however,
they may break off into the joint forming a loose body.
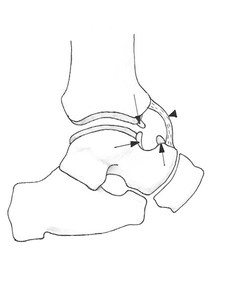
Fig. 1: Diagrammatic representation of the anterior ankle (sagittal) with intra-articular tibiotalar spurs (arrows) and hypertrophied anterior capsular thickening (arrowhead). (Courtesy of Dr Jenna Fielding, Sheffield, UK).
Repetitive supination injuries are also known to cause osteophyte formation secondary to damage to the anterior and medial margin of the articular cartilage.
Another proposed aetiological factor is direct microtrauma caused by ball striking in soccer with direct impact of the ball typically over the anteromedial tibiotalar joint,
where the cartilage is covered only by thin subcutaneous fat4.
All threeBoth mechanisms described occur frequently in soccer players and it is therefore unsurprising that this population of athletes is so commonly afflicted5.
Indeed,
the condition was first described in European soccer players as “footballer’s ankle”5,6.
The theory hypothesised at the time however was one of repetitive traction injury of the anterior joint capsule in extreme plantar flexion causing anterior exostoses.
This is certainly not the case in the anteromedial ankle,
where cadaveric analysis has shown that the bony spurs are intra-articular,
consistent with osteophyte formation7.
The traction hypothesis however may still hold true laterally,
where growth is sometimes extraarticular and may represent enthesophyte formation7.
It is important to remember that the finding of anterior bone spurs does not necessarily mean that the patient is symptomatic.
Studies of asymptomatic athletes have found that a significant proportion (45-59%) have anterior tibiotalar spurs on plain radiograph8.
It is thought that the associated anterior synovial thickening and scarring,
rather than the spurs alone,
are responsible for producing the clinical symptoms9.
Indeed,
post-excision recurrence of the bony spurs is not necessarily accompanied by recurrence of symptoms9,10.
Recent attention has been given to congenital anatomic variants as predisposing factors for the formation of anterior joint space spurs and soft tissue hypertrophy.
A cam-type deformity of the talar dome has been described,
whereby contact between a non-circular arc morphology of the dome with the anterior tibial plafond during dorsiflexion causes abnormal loading of the talar dome cartilage3.
In these patients,
a cavo-varus foot type is more commonly observed,
and the associated external rotation of the tibia is thought to further reduce the tibiotalar joint space3.
In addition,
the orthopaedic literature describes several cases of soft tissue anterior impingement treated successfully by arthroscopic resection of a congenital intraarticular plicae or fibrous bands11,12.
Clinical presentation
The typical symptoms are of chronic anterior ankle pain with subjective feeling of blocking on dorsiflexion.
On examination there is restricted and painful dorsiflexion.
There may also be a palpable soft tissue swelling or a spur over the anterior joint.
The palpable bone spurs are commonly felt over the anteromedial aspect,
while the symptoms of soft tissue impingement are on the anterolateral aspect of the ankle11,13.
Imaging features
Diagnosis of anterior impingement is primarily clinical but conventional,
preferably weight-bearing,
radiographs are useful for the evaluation of bony spurs and the tibiotalar joint space (Fig. 2) .
Anteromedial osteophytes are best demonstrated on the oblique anteromedial impingement (AMI) view14. The plié view (lateral weight-bearing view with the ankle in maximal can demonstrate joint space loss and osseous impingement15.
Radiographic assessment of the tibiotalar joint for secondary signs of degeneration,
particularly joint space loss,
has prognostic importance.
Van Dijk’s radiographic classification system,
based on osteophyte appearance and degree of joint space narrowing,
demonstrated the importance of osteoarthritis as a post-operative prognostic factor16.
Several more recent studies have agreed that secondary osteoarthritis confers a poorer postoperative prognosis9,10.

Fig. 2: Soccer player with clinical anterior impingement. Lateral radiograph shows tibiotalar bony spurs (arrows).
Further imaging is usually unnecessary.
Conventional MRI can be used however to further characterise the location of the spurs within the joint space and to review the degree of synovitis and joint capsule thickening (Fig. 3).
It is also useful to check for concomitant pathology such as osteochondral lesions that may not have been detected on radiography.
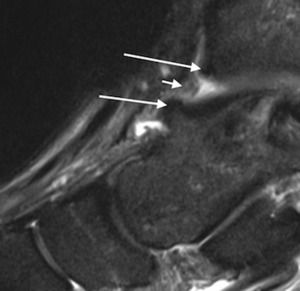
Fig. 3: Sagittal short TI inversion recovery MR image of the ankle of a cricket player shows irregular capsular thickening (short arrow) and anterior tibial and talar spurs (long arrows).
Treatment
- Most patients recover with conservative measures including rest,
activity modification,
and physical therapy.
Particularly in ballet dancers this should be performed in conjunction with correction of technique to correct over-pronation where appropriate.
Ultrasound can be used to direct intaarticular injection of cortisone and local anaesthetic (Fig. 4).
- In resistant cases however surgery has been shown to have a long-term benefit.
In athletes,
arthroscopic resection of the osseous spurs and soft tissue abnormality has shown excellent functional and symptomatic results9.
The overall prognosis after surgery does depend on the degree of degenerative change evident in the rest of the tibiotalar joint at the time of the surgery9,10,17.
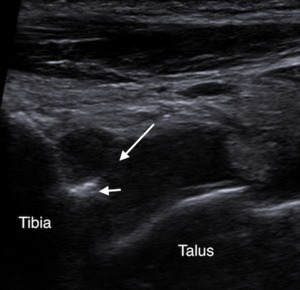
Fig. 4: Sagittal ultrasound of the anterior tibiotalar joint in a rugby player shows hypoechoic synovitis in the anterior joint space (long arrow), and an anterior tibial spur (short arrow). Ultrasound was used to direct inta-articular injection of corticosteroid and local anaesthetic.
Anterolateral impingement syndrome
Anterolateral impingement is well described in the orthopaedic and radiology literature and describes soft tissue hypertrophy and entrapment within the anterolateral recess of the ankle.
It is classically described in young athletic patients following an inversion sprain injury with subsequent chronic anterolateral pain and swelling2.
Anatomy and pathophysiology
The anterolateral recess is a triangular structure bordered posteromedially by the anterolateral tibia and talus and posterolaterally by the anterior fibula.
Anteriorly it is bordered by the anterolateral joint capsule and capsular ligaments.
These include the anterior talofibular,
anterior inferior tibiofibular and calcaneofibular ligaments (Fig. 5).
Ligamentous and capsular tearing and the resultant microinstability and haemorrhage following an ankle sprain may lead to reactive synovial hyperplasia and scarring in the anterolateral gutter18,19.
Compression of the abnormal soft tissue in the anterolateral gutter during dorsiflexion or eversion can cause severe morbidity and pain,
particularly amongst athletes and the younger population.
It is estimated that the incidence of anterolateral impingement syndrome is 3% following ankle sprains4,17.
In advanced cases the soft tissue can become molded to the triangular shape of the anterolateral gutter.
This connective tissue mass was originally described as a “meniscoid lesion” based on its macroscopic meniscus-like appearance20.
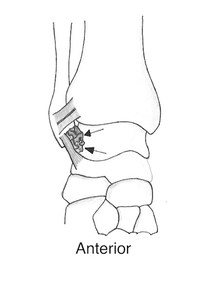
Fig. 5: Diagrammatic representation of the anterior ankle (coronal) indicating the typical location of synovitis (arrows) within the anterolateral recess involving the capsule between the tibiofibular and tibiotalar ligaments in anterolateral impingement syndrome. (Courtesy of Dr Jenna Fielding, Sheffield, UK).
Anterolateral impingement has also been described in a subset of patients with an accessory fascicle of the anteroinferior tibiofibular ligament.
The ligament is invariably multi-fascicular but a discreet inferior fascicle separated from the main body by a fibrofatty septum is variably present (identified in 21-97% of ankles depending on the exact definition) and considered a normal variant18,21.
The accessory fascicle of the anteroinferior tibiofibular ligament (Bassett’s ligament) may normally contact the anterolateral corner of the talus but it is thought that increased contact in dorsiflexion may lead to synovial hypertrophy and impingement within the anterolateral joint space.
Ligamentous abrasion of the exposed anterolateral talar cartilage can sometimes also be seen.
Clinical presentation
The clinical diagnosis of anterolateral impingement is reasonably accurate and based on the anterolateral tenderness,
swelling and pain exacerbated by single leg squatting,
ankle eversion or dorsiflexion.
A provocative physical examination test can be performed in which pressure is applied over the anterolateral ankle while the ankle is brought from the plantar flexed position to full dorsiflexion.
A 94.8% sensitivity and 88% specificity was reported in a prospective study22.
Imaging features
Anterolateral impingement is predominantly a soft-tissue abnormality and therefore radiography and conventional CT have limited specific utility.
Ultrasound and MRI can potentially detect abnormal nodular soft tissue extruding anteriorly from the anterolateral gutter.
In a retrospective evaluation of ultrasound in a small group of elite soccer players with resistant anterolateral impingement awaiting arthroscopy,
synovitic lesions were detected using ultrasound with 100% sensitivity23 (Fig. 6 and Fig. 7).
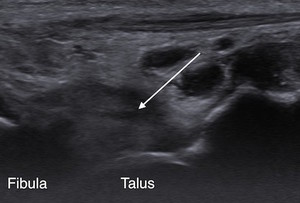
Fig. 6: Rugby league player with previous ankle injuries and persistent anterolateral joint line tenderness. Ultrasound and axial T2w fat suppressed MR image of the ankle showing a synovitic mass in the anterolateral recess (arrow).
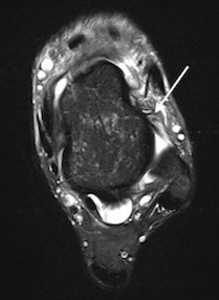
Fig. 7: Rugby league player with previous ankle injuries and persistent anterolateral joint line tenderness. T2w fat suppressed MR image of the ankle showing a synovitic mass in the anterolateral recess (arrow).
MRI has the advantage over ultrasound in being able to assess for whole ankle pathology including co-existing or alternative causes of prolonged ankle pain such as marrow contusions,
chondral lesions,
intra-articular bodies and sinus tarsi syndrome.
MRI can show synovial hypertrophy in the anterolateral recess.
The most reliable sign is the obscuration of the anterolateral recess with scar tissue (Fig. 8 and Fig. 9).
It must be remembered that an abnormal nodular or irregular contour of the recess is commonly found in the asymptomatic population and can merely reflect previous anterolateral trauma or surgery.
The diagnostic ability of MRI in the absence of joint distention with either contrast material or a native effusion remains controversial with some authors previously preferring MR arthrography as it has a reported sensitivity of 97% and specificity of 100%24.
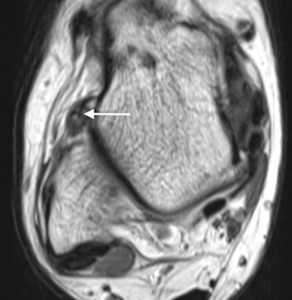
Fig. 8: Rugby league player with a previous lateral ligament injury now presenting with clinical signs of anterolateral impingement. Axial PDw MR image of the ankle showing a synovitic mass in the anterolateral recess (arrows).
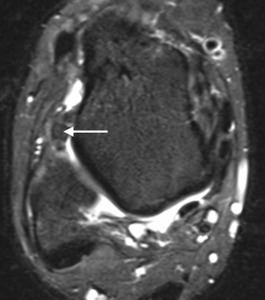
Fig. 9: Rugby league player with a previous lateral ligament injury now presenting with clinical signs of anterolateral impingement. Axial T2w fat suppressed MR image of the ankle showing a synovitic mass in the anterolateral recess (arrows).
However,
with advances in MRI hardware technology,
MR arthrography is now largely redundant and,
with sufficient experience,
the diagnosis can be made on conventional MRI with relative confidence (75-83% sensitivity and 75-100% specificity,
depending on the experience of the reporter)26. T1-weighted images were deemed the most useful for detecting the intermediate to low signal hypertrophy and scarring in the anterolateral gutter25.
Sagittal T1-weighted images are a useful adjunct,
demonstrating anterior displacement of the normal hyperintense fat anterior to the fibula by the hypointense scar tissue.
Specificity however for all these findings on ultrasound or MRI is poor,
particularly with regards to the detection of thickened non-enhancing scar tissue.
Treatment
- The initial treatment is conservative,
with immobilization,
physiotherapy and nonsteroidal anti-inflammatory medication.
Dry needling of the abnormal soft tissue with an intaarticular injection of cortisone and local anaesthetic may be performed under ultrasound guidance,
allowing a return to previous levels of activity,
even in elite athletes,
but this technique has not been fully evaluated in the literature.
- If these measures fail,
arthroscopic evaluation and resection of hypertrophied synovium and scar tissue,
including the distal fascicle of the anterior tibiofibular ligament when that is the underlying etiology,
has yielded good to excellent symptomatic and functional results26,27.
Anteromedial impingement syndrome
Anteromedial impingement is an uncommon cause of chronic ankle pain and usually occurs alongside other pathology including anterior or anterolateral impingement and chondral lesions.
Classic findings include hypertrophic spurs,
reactive fibrosis and synovial proliferation along the anteromedial gutter of the tibiotalar joint.
Anatomy and pathophysiology
Although originally thought to result from a pronation (eversion) injury with traction on the anterior tibiotalar ligament of the deltoid complex,
it is now believed to be a rare consequence of a supination (inversion) injury,
probably with a rotational component,
causing microtrauma and tearing of the anteromedial capsule and tibiotalar ligament16,25 (Fig. 10).
The resulting capsular,
ligamentous and synovial hypertrophy and thickening can become compressed during dorsiflexion and inversion.
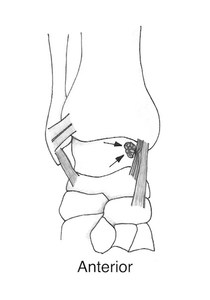
Fig. 10: Diagrammatic representation of anteromedial ankle impingement with a ‘meniscoid’ lesion (arrows), and a thickened anterior tibiotalar ligament. (Courtesy of Dr Jenna Fielding, Sheffield, UK).
Clinical presentation
The diagnosis is usually a clinical one,
characterised by anteromedial ankle pain on dorsiflexion and inversion.
There is tenderness and swelling along the anteromedial joint line and sometimes restriction of movement and palpable marginal osteophytes on examination.
Imaging features
If bone spurs are suspected the anteromedial impingement view radiograph can be useful14.
MRI features include post-traumatic synovitis,
synovial hyperplasia,
capsular thickening and scarring of the anterior tibiotalar ligament (Fig. 11 and Fig. 12)28.
There are however no large imaging studies of anteromedial impingement.
The largest surgical series involved 22 females actively involved in competitive gymnastics and demonstrated that 86% had concomitant ankle lesions found at arthroscopy29.
MRI therefore has added value in assessing for related concomitant pathologies.
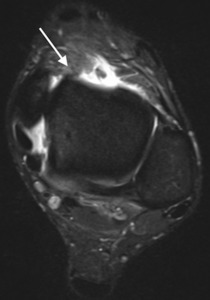
Fig. 11: Rugby league player with anteromedial impingement. Axial T2w fat suppressed MR image with irregular soft tissue thickening within the anteromedial ankle joint (arrow).
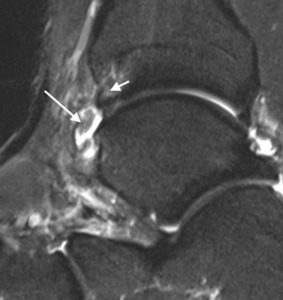
Fig. 12: Rugby league player with anteromedial impingement. Sagittal T2w fat suppressed MR image with abnormal capsular thickening (long arrow) and bone marrow oedema in the anteromedial spur on the distal tibia (short arrow).
Treatment
There are no accounts in the literature of management with purely conservative measures,
but these typically involve physiotherapy and heel lifts to improve ankle joint biomechanics30,31.
One group uses an anaesthetic-only injection at the area of presumed impingement with the patient re-assessed clinically a few hours later29.
Those with a favourable response in terms of pain and mobility return for a localised ultrasound guided soft tissue steroid injection (Fig. 13).
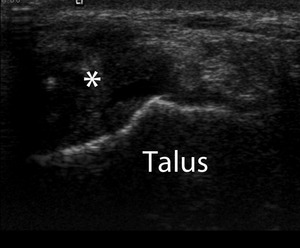
Fig. 13: Axial ultrasound image demonstrating nodular hypoechoic synovitis (*) in the anteromedial ankle in a patient with clinical signs of anteromedial impingement. Ultrasound was used to direct inta-articular injection of corticosteroid and local anaesthetic.
Surgical osteophyte and soft tissue debridement may give symptomatic relief and functional improvement.
In a group of 22 female gymnasts with refractory anteromedial impingement pain,
64% returned to competitive gymnastics following surgery29.
Murawski and colleagues reported good or excellent functional outcomes in 91% of their series of 100 arthroscopic debridements (age range 13 – 60) with a 5% complication rate and mean return to play in the athletic sub-population of seven weeks32.
Posteromedial impingement
Posteromedial ankle impingement is thought to occur as a consequence of a severe inversion injury.
Although there are few reported series in the literature,
the identified soft tissue imaging findings on ultrasound and MRI are relatively characteristic33,34,35.
Anatomy and pathophysiology
First described in a surgical case report in 1993,
posteromedial impingement has become recognised as an uncommon consequence of severe ankle inversion injury in which the deep fibres of the posterior tibiotalar ligament and the posteromedial capsule become compressed between the medial wall of the talus and posterior margin of the medial malleolus (Fig. 14)33,35,36.
Inadequate healing and fibrosis can cause painful chronic posteromedial joint impingement.
The abnormal hypertrophic soft tissue may displace or encase the surrounding tendons,
particular the posterior tibialis tendon34,35.
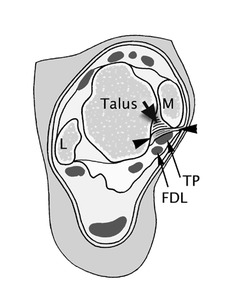
Fig. 14: Axial illustration shows structures involved in posteromedial impingement. M, medial malleolus; TP, tibialis posterior tendon; FDL, flexor digitorum longus tendon; L, lateral malleolus. Arrow-heads donate posterior fibres of tibiotalar ligament; short arrow indicates deep fibers of tibiotalar ligament (Ref 35).
Clinical presentation
Patients usually present with posteromedial pain,
which may occur gradually once the precipitating anterolateral inversion injury signs have resolved.
The pain is exacerbated by provocative testing,
by palpating the site while moving the ankle into plantar flexion and inversion.
This clinical sign helps to distinguish posteromedial impingement from pure posterior tibialis tendon dysfunction.
Imaging features
Ultrasound and MRI have been described in three case series but MRI is the imaging modality of choice as it permits identification of coexisting anterolateral and posteromedial capsule ligament lesions and particularly associated osteochondral lesions1,33-35.
Axial PD and T2-weighted sequences show loss of striation of the posterior tibiotalar ligament,
capsular thickening and oedema around the posteromedial tendons (Fig. 15 and Fig. 16).
Messiou and colleagues demonstrated that,
of nine elite athletes with clinical posteromedial impingement,
there was signal abnormality in the posterior tibiotalar ligament in all cases,
displacement of the posterior tibialis tendon and flexor digitorum tendon in seven cases and disruption of the posterior tibiotalar ligament fibres in four cases35.
Posteromedial tendon encasement was more common in chronic cases.
No specific pattern of marrow oedema has been described.
As with other impingement syndromes,
MRI findings are non-specific,
with mild synovitis and thickening sometimes found in asymptomatic cases.
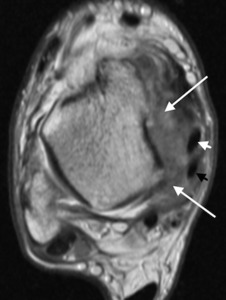
Fig. 15: Volley ball player with posteromedial impingement. Axial PDw MR image shows disorganisation of the deltoid and posteromedial tissues with scarring and soft tissue thickening (long arrows) displacing the tibialis posterior (white short arrow) and flexor digitorum longus (black short arrow) tendons.
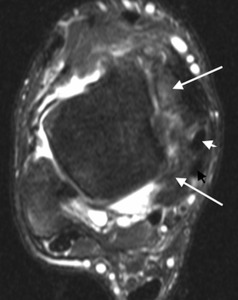
Fig. 16: Volley ball player with posteromedial impingement. Axial T2w fat-suppressed MR image shows disorganisation of the deltoid and posteromedial tissues with scarring and soft tissue thickening (long arrows) displacing the tibialis posterior (white short arrow) and flexor digitorum longus (black short arrow) tendons.
Symptomatic patients with isolated posteromedial synovitis and no associated chondral or ligamentous instability may benefit from ultrasound-guided therapeutic injection.
Ultrasound findings include hypoechoic posteromedial capsular thickening deep to and sometimes displacing the tibialis posterior tendon,
obscuring the striated detail of the posterior tibiotalar ligament (Fig. 17)35.
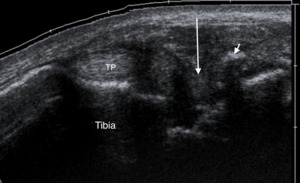
Fig. 17: Volley ball player with posteromedial impingement. Axial oblique ultrasound of the posteromedial ankle showing hypoechoic soft tissue thickening (long arrow) within the posteromedial recess and around tibialis posterior (TP) tendon with dystrophic calcification (short arrow).
Treatment
- If conservative measures have failed,
ultrasound can be used to identify the capsular abnormality and guide percutaneous dry needling and injection of steroid and local anaesthetic.
This approach allows a return to previous levels of activity in elite athletes.
In Messiou’s study,
all athletes returned to pre-injury activity within three weeks35.
- For resistant cases,
successful outcome has been reported following surgical resection of abnormal posteromedial soft tissue without ligamentous repair33,34.
Posterior impingement
Posterior ankle impingement is a common cause of posterior ankle pain in sports that involve repetitive hyper-plantar flexion.
It has been extensively described in ballet dancers (due to the ‘en pointe’ or ‘demi-pointe’ positions),
in football players (when kicking the ball),
cricket players and javelin throwers (front foot planting while throwing or bowling),
and horizontal jump athletes (lead foot on toe-off)37,38.
Albisetti and colleagues identified a prevalence of 6.5% during a one-year observation of 186 ballet dance trainees40.
Injury audit data from the English Cricket Board revealed that posterior ankle impingement was the most common cause for players deemed unfit to train or play secondary to foot and ankle problems over the 2001 - 2002 season.
It principally affects the front foot of fast bowlers and represented more days lost for injury to foot and ankle pathology that season than to lateral ankle ligament and Achilles tendon pathologies combined40.
Other names,
such as “os trigonum syndrome”,
“talar compression syndrome” and “posterior block” have also been attributed to this collective syndrome of pathologies,
all.
All of which are characterised by forced or repeated ankle plantar flexion with subsequent compression of bone or soft tissues between the posterior articular lip of the tibia and the calcaneus4,17.
Anatomy and pathophysiology
There are many causes of posterior impingement,
including bone lesions,
soft tissue lesions and anomalous and accessory muscles.
The posterior talar process has two posterior projections or tubercles.
These form a fibro-osseous groove through which the flexor hallucis longus tendon runs.
The lateral tubercle (or posterolateral process) is larger than the medial one and contains a secondary ossification centre.
This usually mineralises between 7 - 13 years of age and fuses by one year.
In 7% – 14% of adults it remains as a separate accessory bone,
the os trigonum,
and is bilateral in 1.4% of cases (Fig. 18)41.
This structure is usually asymptomatic but may become painful if there is disruption of the synchondrosis leading to a cycle of inflammation and soft tissue hypertrophy.
Alternatively,
chronic stress may lead to a fracture.
An elongated posterolateral process of the talus,
(Steida or trigonal process),
can also be important in posterior impingement (Fig. 19).

Fig. 18: Osseous anatomical structure of the talus associated with posterior impingement. Sagittal T2w fat suppressed MR image shows an os trigonum with patchy increased signal around the synchondrosis due to normal intrinsic vascularity (long arrow) and down-sloping posterior tibia (short arrow).
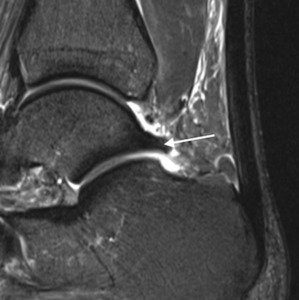
Fig. 19: Osseous anatomical structure of the talus associated with posterior impingement. Sagittal T2w fat suppressed MR image shows a Steida process (arrow).
Another anatomical consideration is the morphology of the posterior articular surface of the tibia (posterior malleolus) and the calcaneal tuberosity.
A more down-sloping configuration of the posterior malleolus or a prominent posterior process of the calcaneusm may be contributory42.
Soft tissue impingement between the posterior tibial plafond and the superior aspect of the calcaneusm typically involves scarring and oedematous thickening of the posterior capsule.
The supporting posterior talofibular,
tibiofibular and intermalleolar ligaments can also get compressed but are rarely primarily abnormal.
It is hypothesised that subclinical thickening exists in many athletes and any acute injury to the ankle that produces haemarthrosis can cause further thickening that may explain why many athletes present during rehabilitation for a seemingly previous remote acute injury43.
The flexor hallucis longus tendon can also become secondarily involved with tendinopathy and tenosynovitis with symptoms that can mimic impingement.
The posterior intermalleolar ligament is an anatomical variant of the posterior ligaments of the ankle.
First described by Rosenberg and colleagues in 1995,
it was identified in 56% of cadaveric specimens44.
The ligament extends obliquely from the posterior margin of the medial malleolus to the superior margin of the fibular malleolar fossa.
It lies in between the inferior tibiofibular ligament and the posterior talofibular ligament.
When the foot is in plantar flexion,
the posterior intermalleolar ligament can protrude into the joint and become entrapped and torn.
Bucket handle tears and entrapment of the ligament have been described as a cause of posterior impingement in ballet dancers45.
Although the presence of a posterior intermalleolar ligament is common,
posterolateral impingement related to it is rare.
In addition,
generalized hypermobility or talocrural laxity relating to previous anterior talofibular ligament disruption can also put stress on the posterior capsule-ligament complex and predispose to posterior impingement37.
Clinical presentation
Presentation is usually with progressive posterior ankle pain but diagnosis can be difficult as it may mimic other pathologies such as Achilles,
flexor hallucis or peroneal tendon pathology.
Like other ankle impingement symptoms it can present subacutely after a seemingly remote acute ankle injury as the athlete rehabilitates.
The pain is aggravated by running,
kicking,
jumping or cutting manoeuvres,
and with either plantar or dorsiflexion due to either compression or stretching of the abnormal posterior soft tissue.
Pain relating to an os trignonum or Stieda process is more often posterolateral,
whereas flexor hallucis issues are more commonly posteromedial46.
It is often difficult however to clinically localise the pain to a side.
On examination,
impingement testing by applying passive plantar flexion to the ankle with the patient lying in the prone position and the knee flexed is invariably positive.
Involvement of the flexor hallucis longus tendon is suspected if resisted isometric plantar flexion of the first metatarsal phalangeal joint results in posterior ankle pain.
Imaging features
Plain radiography is the first step in identifying the os trigonum or Steida process osseous variants.
It should be remembered however that symptom severity is not related to the size or even the presence of these two structures47.
The shape of the posterior malleolus and the calcaneal tuberosity can also be assessed.
Sagittal T1-weighted and fat-supressed fluid sensitive sequences allow optimal visualisation of an os trigonum,
a Steida process,
a down-sloping posterior malleolus or prominent calcaneal tubercle.
Bone marrow oedema may be seen in all these osseous structures and fluid signal may be seen at the synchondrosis within a non-united fracture.
However this latter feature must be carefully evaluated,
as a normal synchondrosis will show patchy increased T2-weighted signal due to normal intrinsic vascularity (Fig. 18).
Axial and sagittal fat-supressed fluid-sensitive images allow visualisation of soft tissue abnormalities such as posterior capsular thickening,
ligament disruption,
flexor hallucis tenosynovitis and soft tissue oedema and synovitis48,49.
The combined presence of bone marrow oedema and posterior ankle synovitis suggests a diagnosis of posterior ankle impingement (Fig. 20 and Fig. 21)50.
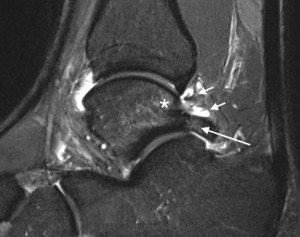
Fig. 20: Posterior impingement. Sagittal T2w fat suppressed MR image of posterior ankle impingement with posterior capsular synovitis (short arrows). There is low grade oedema in the os trigonum (long arrow), and posterior body of the talus (*).
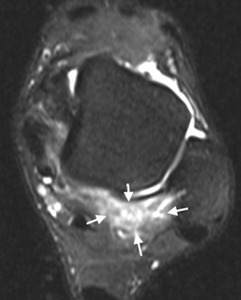
Fig. 21: Posterior impingement. Axial T2w fat suppressed MR images of posterior ankle impingement with posterior capsular synovitis (short arrows).
As with other ankle impingement syndromes,
MRI is used to look for other related pathologies or unrelated mimics,
such as Achilles tendinopathy,
subtalar arthritis,
flexor hallucis tenosynovitis,
Haglund’s deformity,
retrocalcaneal bursitis,
and osteochondral lesion.
Ultrasound is increasingly being used to demonstrate the hypoechoic nodularity of capsular thickening around the lateral aspect of the posterlateral process or os trigonum.
The main role however is to target percutaneous therapy.
Treatment
- Initial management is conservative with taping and bracing to limit plantar flexion,
followed by manual mobilisation and anti-inflammatory medication.
An injection of local anaesthetic into an os trigonum synchondrosis under fluoroscopic guidance can be a useful diagnostic adjunct and can help therapeutically where there is a flare-up during a performance season46.
If symptoms persist,
an ultrasound guided injection of corticosteroid and local anaesthetic into the abnormal area of soft tissue with dry needling can be useful,
particularly in the absence of an os trigonum43.
- If symptomatic osseous impingement fails to resolve,
operative management is advised.
Surgical excision of osseous and soft tissue elements have a high success rate in returning athletes back to their sport of choice46.
Extra-articular lateral hindfoot impingement
Severe pes planus and hindfoot valgus deformity can lead to extra-articular lateral hindfoot impingement,
including talocalaneal and subfibular impingement.
This can present with progressive lateral ankle pain and deformity.
Anatomy and pathophysiology
Valgus deformity of the ankle is associated with a shift of weight-bearing force from the talar dome to the lateral talus and fibula.
Subsequent talocalcaneal impingement may follow,
with or without subfibular impingement.
This may occur secondary to malunion after calcaneus fracture,
posterior tibialis tendon dysfunction,
neuropathic arthropathy or inflammatory athritides52.
Clinical presentation
Regardless of the initial cause of flatfoot,
patients with rigid flatfoot deformity experience decreased range of motion at the midfoot and hindfoot and decreased ankle dorsiflexion52,53.
Although the pain may initially locate to the medial ankle in cases of posterior tibialis tendon dysfunction,
lateral ankle pain predominates in chronic severe dysfunction54.
Further midfoot and hindfoot pain is associated with secondary degeneration and progressive deformity.
Imaging features
Weight-bearing radiographs are useful to assess the plantar arch and hindfoot valgus.
Although there are no definite radiographic criteria for lateral hindfoot impingement,
subfibular osseous impingement should be suspected if the distance between the fibula and the lateral process of the talus on the anteroposterior view measures 1 mm or less (Fig. 22)55.

Fig. 22: Patient with pes planus, hindfoot valgus following a calcaneal fracture who presented with lateral hindfoot tenderness. Frontal radiograph shows close approximation of the fibular tip with the calcaneus (arrows).
CT can also be used and is similarly suspicious if there is a bony protrusion of 2 mm or more at the lateral surface of the talus on axial view or if bone spurs are seen on the lateral process of the talus and on adjacent fibula on coronal view (Fig. 23)55.
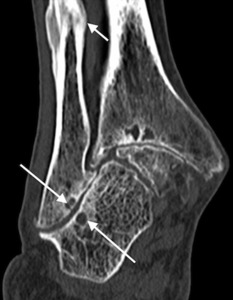
Fig. 23: Severe hindfoot valgus in a patient with Rheumatoid arthritis. There is pseudoarticulation between the fibula and calcaneus with sclerosis, articular irregularity and extensive cystic change (long arrows). Also, an associated chronic diaphysial fracture of the distal fibula (short arrow)
MRI may show marrow oedema or sclerosis at the posterior subtalar joint,
fibular tip,
lateral process of the talus and lateral calcaneus (Fig. 24).
There may also be thickening of the subfibular soft tissues with calcaneofibular ligament entrapment and subluxation of the peroneal tendons52. MRI is also used to check for posterior tibialis tendinopathy and other associated sources of pain such as lateral bursitis and distal fibular stress fractures.an be used to assess for other associated sources of pain,
such as lateral bursitis and distal fibular stress fracture.
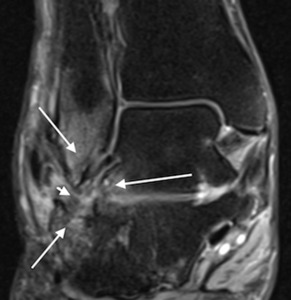
Fig. 24: Patient with pes planus, hindfoot valgus following a calcaneal fracture who presented with lateral hindfoot tenderness. Coronal PDw MR image (B) shows extra-articular sub-fibular impingement with bone marrow oedema in the fibular tip and lateral margins of the talus and calcaneus (long arrows). There is associated soft tissue oedema and synovial thickening (short arrow).
Treatment
- Conservative early measures are directed at preventing further osseous deformity with physiotherapy and orthotics.
- Surgical correction of hindfoot deformity is however usually required and consists of either calcaneal osteotomy or in the most severe cases,
arthrodesis.

 with intra-articular tibiotalar spurs (arrows) and hypertrophied anterior capsular thickening (arrowhead). (Courtesy of Dr Jenna Fielding, Sheffield, UK).")
.")
 and anterior tibial and talar spurs (long arrows).")
, and an anterior tibial spur (short arrow). Ultrasound was used to direct inta-articular injection of corticosteroid and local anaesthetic.")
 indicating the typical location of synovitis (arrows) within the anterolateral recess involving the capsule between the tibiofibular and tibiotalar ligaments in anterolateral impingement syndrome. (Courtesy of Dr Jenna Fielding, Sheffield, UK).")
.")
.")
.")
.")
, and a thickened anterior tibiotalar ligament. (Courtesy of Dr Jenna Fielding, Sheffield, UK).")
.")
 and bone marrow oedema in the anteromedial spur on the distal tibia (short arrow).")
 in the anteromedial ankle in a patient with clinical signs of anteromedial impingement. Ultrasound was used to direct inta-articular injection of corticosteroid and local anaesthetic.")
.")
 displacing the tibialis posterior (white short arrow) and flexor digitorum longus (black short arrow) tendons.")
 displacing the tibialis posterior (white short arrow) and flexor digitorum longus (black short arrow) tendons.")
 within the posteromedial recess and around tibialis posterior (TP) tendon with dystrophic calcification (short arrow).")
 and down-sloping posterior tibia (short arrow).")
.")
. There is low grade oedema in the os trigonum (long arrow), and posterior body of the talus (*).")
.")
.")
 shows extra-articular sub-fibular impingement with bone marrow oedema in the fibular tip and lateral margins of the talus and calcaneus (long arrows). There is associated soft tissue oedema and synovial thickening (short arrow).")
. Also, an associated chronic diaphysial fracture of the distal fibula (short arrow)")