1.
OSTEOCHONDRAL FRACTURE
Osteochondral fracture of the talar dome is the commonest missed fracture associated with inversion sprains.
It may be staged in 4 types of injury: from an undislocated compression fractures of the subchondral bone to a complete detachment and displacement of the fibro-osseous fragment.
The main imaging findings in MRi is the detection of a crescentic fracture line and a focal cartilage lesion,
with adjacent bone marrow edema.
In unstable osteochondral fractures we may find a high signal line demarcating the osteochondral fragment from the bone or the presence of sunchondral cysts.
Both x-rays and CT are able to detect displaced defects.
However,
they are insensitive in grading lower stage lesions and are inadequate in predicting stability.
The main places of these injuries are the talar or tibial articular surfaces but most frequently involve the lateral or medial talar dome.

Fig. 1: Male adult with chronic ankle pain six months after a sprain. A and B) COR T2 FS. Osteochondral lesion in the posteromedial portion of the talar domus and adjacent bone marrow edema. No signs of instability fragment.
2. ANKLE IMPINGEMENT
Sprain is the leading cause of impingement syndromes.
Soft tissue and osseous impingement syndromes of the ankle are a potential cause of chronic post- traumatic pain.
Frequently,
this event results from an inversion injury,
with a consequent injury to the lateral ligaments and / or syndesmosis causing proliferation of soft tissue in the anterolateral gutter.
There may be also lesions to the medial ligament complex (deltoid),
causing a medial fibrocicatricial proliferation.
This tissue may impact the osseous surfaces,
with osteophytes formation,
best seen on lateral view and a sagittal plane.
MRI may show marrow edema at impaction sites.
Patients present chronic pain and anterolateral swelling and limits dorsiflexion.
MRI may exclude the differentials as chondral defect,
osteochondral lesions,
intraarticular bodies,
spinal cord injuries.
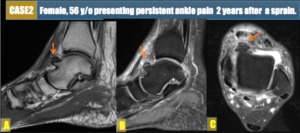
Fig. 2: (A, B, C) SAG T1 and T2 FS and AX T2 FS shows proeminent osseous hypertrophy in the anteromedial aspect of the talar neck, with bone marrow edema and a tibiotalar effusion, with reacional synovitis, those findings are consisting of an anteromedial impact syndrome.
�
3.
SYNDESMOTIC INJURY
A tibiofibular syndesmotic sprain or high ankle sprains,
are less common following a trauma,
but syndesmotic injury is another recognised cause of prolonged ankle pain and disability.
This injury would result in oedema around or within the tibiofibular ligament on MRI and in the sindesmosis.
Given the increased severity and long-term sequelae of syndesmotic injuries,
this diagnosis must always be excluded in imaging examinations.

Fig. 6: AX T1, SAG T2 FS and COR T2 FS MRI ankle images shows a subcortical oblique fracture of the posterior tibial protuberance (A) with edema of the adjacent bone marrow .
There is intense tibiofibular syndesmosis edema (C) without significant diastesis. Joint effusion, synovitis with signs reaction (B).
4.
SINUS TARSI SYNDROME
The most common cause of sinus tarsi syndrome is ankle sprain,
and this syndrome is another important cause of a persistent pain after a sprain.
It can be recognized in MRI by an alteration of the normal fat signal of the sinus tarsi with decreased signal intensity on T1- and T2-weighted images,
which correlates with fibrosis,
resultant from rupture of cervical ligament.
This scar tissue formation causes pain,
subjective impingement and instability.
Also,
heterotopic ossification may also develop.
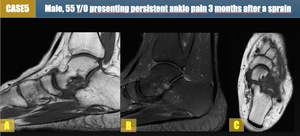
Fig. 3: MRI SAG T1, T2 FS and AX T1 shows edema and obliteration of the tarsal sinus fat.
5.
MISSED FRACTURE
The second most commonly missed fractures (after osteochondral fractures) involves the lateral talar process.
CT readily shows this injury.
Failure to detect this fracture can have severe consequences: the fracture is intra-articular and mainly affects a young age group,
and so may fail to heal,
resulting in non-union and chronic pain.
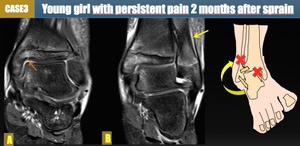
Fig. 4: (A, B) COR T2 FS images showing an incomplete fracture of medial malleolus extending through the epiphyseal plate with bone marrow edema and subperiosteal hematoma (yellow arrow in B). The patient had a previous normal X-ray examination at the time of the sprain. Findings are consisting with an occult fracture.
�
6.
SYMPATHETIC DYSFUNCTION
It is characterised by extreme burning pain,
a history of trauma and evidence of sympathetic dysfunction.
Most patients describe a previous injury that can be minor or severe,
and this includes sprains.

Fig. 5: COR T1, COR T2 FS and AX T2 FS MRI foot images shows diffuse edema in tarsal bones in a patient presenting pain and sensitive alteration in the foot. Also notice a fracture in the base of the fifth metatarsal.
