Authors:
E. Sellon, P. Robinson; Leeds/UK
DOI:
10.1594/essr2016/P-0119
Background
Introduction
- Muscle injuries are a common consequent of sport and usually arise from direct blunt impact or indirectly from the application of excessive eccentric force.
- They do not always require imaging but do need to be accurately diagnosed and characterised in order to optimise athletic performance and to predict recovery time.
- Although more prevalent in the lower limb,
muscle-tendon unit injuries to the chest wall and upper limb are well described and represent a significant cause of time away from sport,
particularly in weight lifting and contact sports such as rugby,
wrestling and American football.
Ultrasound technique
Linear high frequency probes are most commonly used (9-17MHz) and provide excellent near field resolution.
In the upper limb low frequency probes are rarely required.
The advent of extended field of view (FOV) imaging allows the user to produce images that most clinicians and patients can clearly understand. Colour or power Doppler can be used to demonstrate increased blood flow at the injury site.
Dynamic examination while manoeuvring the injured arm can help clarify the diagnosis.
It is often helpful to compare appearances with the contralateral side.
MRI technique
Muscle injury protocols vary but should include a fluid sensitive sequence (i.e.,
fat-suppressed T2-weighted or proton density-weighted turbo spin echo and STIR sequences) for detecting oedematous change.
T1-weighted turbo spin echo is used to visualise fatty infiltration and to differentiate between haemorrhage and oedema.
T1-weighted imaging also better defines the muscle anatomy for locating the anatomical site of injury. Contrast is rarely required (Fig. 1).
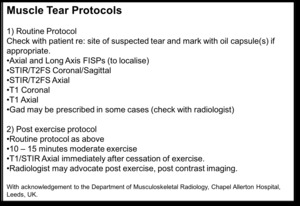
Fig. 1: ESSR sports sub-committee MRI imaging protocol for muscle tears. Reproduced with permission from Department of Musculoskeletal Radiology, Chapel Allerton Hospital, Leeds, UK.
Emerging techniques
Several advanced techniques including diffusion tensor imaging,
elastography and spectroscopy have been used to assess skeletal muscle but are not commonly used in current clinical practice.
Of these,
muscle fibre tracking with diffusion tensor imaging (DTI) has proved the most promising in injury assessment.
It is used in the research setting to study muscle architecture and microstructure by creating three-dimensional morphological reconstructions.
Normal muscle on DTI demonstrates uniformity in fibre and axis orientation1,
but when injured,
fibre uniformity is disturbed.
The degree of muscle fibre derangement and the pennation angle of the fibres against the force-generation axis can be measured2,3.
