Content:
(1) Common sports related muscle injuries; (a) contusions (and myositis ossificans,
(b) laceration,
(c) strain and tear,
(d) delayed onset muscle soreness,
(e) compartment syndrome. (2) Specific muscle injuries; (a) Pectoralis major,
(b) Pectoralis minor,
(c) Shoulder and upper arm,
(d) Elbow and lower arm (Fig. 2).

Fig. 2: Content page
Common sports related muscle injuries
Contusion
This type of injury is usually caused by direct,
blunt trauma and usually occurs deep in the muscle belly. In the upper limb they may also be associated with shoulder instability.
This is well described in the dynamic stabiliser muscles of the shoulder in rugby players following either direct lateral impact in the tackle or forced abduction and external rotation in the try scoring position.
Ultrasound imaging reveals discontinuity of normal muscle architecture,
with ill-defined hyperechogenicity that may cross fascial boundaries4.
MR imaging typically shows focal high signal intensity on fluid sensitive sequences,
with a diffuse or geographic appearance,
often with a feathery margin involving more than one muscle which is rare in strain injury (Fig. 3).
Contusions can look very similar to strain (non-contact) injuries but are less symptomatic and confer a significantly shorter recovery time and therefore need to be diagnosed with close attention to the clinical history5.
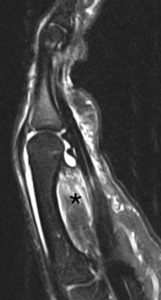
Fig. 3: International cricket player with a painful hand after ball strike. Sagittal T2w fat suppressed MR image showing marked oedema (asterisk) spreading across the lumbrical muscles on the palmar aspect of the hand.
With sufficient force,
focal oedema may be accompanied by an intramuscular haematoma.
Acute haematomas appear hypoechoic with hyperechogenicity of the surrounding muscle.
In the early sub-acute phase,
they may solidify and become isoechoic with muscle making assessment more difficult.
After 48-72 hours the haematoma develops into a clearly defined hypoechoic collection with an echogenic margin which eventually fills in.
If the clinical and imaging features are uncertain,
contrast can be given to help differentiate a simple haematoma from a haemorrhagic neoplasm.
Muscle haematomas also follow a predictable pattern of appearances on MR imaging with the signal characteristics changing depending on the nature of the predominant blood product.
There may also be enlargement of the involved muscle.
It is reported that the ideal time for imaging is between 2 and 48 hours post injury as this allows time for the haematoma to form but not spread outside the muscle6.
Myositis ossificans and myonecrosis are potential complications of contusion.
Myositis ossificans has been reported particularly in the brachialis muscle and may follow a contusion,
sprain or overuse injury7.
Peripheral haematoma calcification may be visible on CT and plain radiographs at approximately six weeks and ossification occurs by six months8. Focused US assessment however is more sensitive than this and may detect early myositis ossificans at 3 weeks post injury (Fig. 4, Fig. 5, Fig. 6,
Fig. 7).
Myonecrosis may appear similar to an intramuscular haematoma but should particularly be considered following a history of penetrating trauma.

Fig. 4: Myositis ossificans. (A) Radiograph shows a soft tissue mass (asterisk) with classical peripheral calcification (arrows).
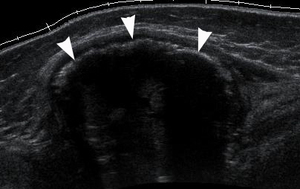
Fig. 5: Myositis ossificans. Longitudinal ultrasound confirms calcification (arrowheads) with posterior acoustic shadowing and normal surrounding tissue planes.
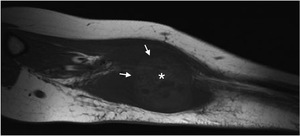
Fig. 6: Myositis ossificans. Sagittal T1w MR image displays a heterogeneous and oedematous mass (asterisk) with peripheral low signal calcification (arrows) and marked surrounding oedema.
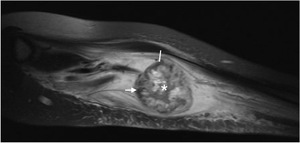
Fig. 7: Myositis ossificans. T2w MR images display a heterogeneous and oedematous mass (asterisk) with peripheral low signal calcification (arrows) and marked surrounding oedema.
Laceration
Direct upper limb muscle trauma may rarely involve a laceration.
In the chest and upper limb there is particular risk of neurovascular injury.
The deep extent of lacerations can be difficult to assess clinically and radiologically and are often initially underestimated9. If there are overlying wound dressings limiting US assessment,
MR imaging is preferred and can better localise neurovascular structures.
Strain and tear injury
Strains and tear injuries typically involve the musculotendinous junction following passive stretching or eccentric activation of a muscle.
They typically affect muscles that extend across two joints and have a high proportion of fast twitch (type II) fibres.
In the chest wall and upper extremity this includes pectoralis major,
particularly in weight lifters and rugby players,
latissimus dorsi in overhead throwing athletes and forearm flexor-pronators in baseball pitchers (Fig. 8).
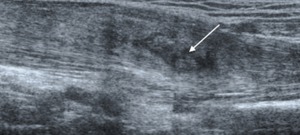
Fig. 8: Pronator teres contusion. Longitudinal ultrasound shows a mixed echogenicity haemorrhage within the muscle belly (arrow).
Musculotendinous strains are clinically classified as grade 1,
2 or 3 based on absent,
mild or complete loss of muscle function respectively10.
This grading system,
devised by O’Donoghue in 1962 is relatively crude,
does not account for associated tendon injury and does little in itself to predict recovery time11.
Some prognostic studies,
concentrating on hamstring injuries,
have proposed that longer recovery times are associated with a larger volume of affected muscle,
greater longitudinal extent and percentage cross-sectional area of muscle oedema,
more proximal injury site and the presence of a haematoma12.
This has not been successfully quantified or extrapolated to other muscle groups.
One group have proposed a classification system based on imaging findings that includes detail on whether the injury is proximal,
middle or distal and whether it is predominantly intramuscular,
myofascial,
perifascial or myotendinous in location to help predict recovery time,
but this has yet to be validated clinically and has focussed on lower limb injuries 3.
On US imaging,
grade 1 injuries typically appear normal.
Grade 2 injuries demonstrate discontinuity of the echogenic perimysial striae either at the musculotendinous or at the myofascial junction,
particularly on dynamic testing.
There may also be an intramuscular haematoma.
Grade 3 injuries are characterised by complete rupture of the muscle at the musculotendinous junction.
Intramuscular collections are common.
On MR imaging,
grade 1 injuries reveal interstitial oedema and haemorrhage at the musculotendinous junction with a feathery intramuscular pattern as it extends into the adjacent muscle fascicles.
Grade 2 injuries are characterised by architectural distortion with haematoma.
Grade 3 injuries are complete disruptions of the musculotendinous unit with haematoma filling the space.
Delayed onset muscle soreness
Delayed onset muscle soreness (DOMS) results from unaccustomed exercise,
particularly involving eccentric contractions.
It may occur in elite athletes during pre-season training or early in the strength and conditioning phase of injury rehabilitation.
Muscle soreness typically has a gradual onset 1 to 3 days post activity and is self-remitting.
It is important only in that it may mimic a muscle sprain on imaging which may also be a clinical concern with athletes rehabilitating post injury.
US may be normal or may demonstrate geographic hyperechogenicity affecting several muscles across different compartments.
It is less prone to targeting the musculotendinous junction but may not be distinguishable from a strain injury on imaging alone.
MR imaging demonstrates diffuse T2-weighted or STIR hyperintense muscle oedema with the same pattern of distribution.
Compartment syndromes
When severe,
muscle oedema can result in exertional rhabdomyolysis and elevated compartment pressures that are sustained after exercise and cause pain and swelling (Fig. 3).
When acute this may require urgent fasciotomy.
Chronic exertional compartment syndrome is similarly caused by increased compartment pressures during exercise but resolve between episodes.
Clinically,
patients present with a throbbing pain that is exacerbated by palpation or passive stretching.
In the upper limb this has been most frequently reported in climbers,
gymnasts,
tennis players and motocross racers.
MR imaging may be obtained pre and post exercise (squeezing a rubber ball or hand grip) with persistent oedema at 15 to 20 minutes post exercise acting as a surrogate marker for raised compartment pressures.
However,
some clinicians believe that imaging can predict or confirm diagnosis so caution should be conveyed in reporting and case discussions that this remains a clinical diagnosis.
Specific Muscle Injuries
Pectoralis major strain
The pectoralis major is the largest and most superficial muscle in the anterior chest wall and is predominantly composed of type II muscle fibres.
It is an extremely powerful adductor,
internal rotator,
and flexor of the humerus and acts as an important dynamic stabiliser of the shoulder.
Pectoralis major has a complex anatomical arrangement,
shaped like a fan with a trilaminar tendon sheath (Fig. 9).
The laminae originate from the medial clavicle,
the sternum and the aponeurosis of the external oblique muscle and the cartilages of the first six ribs.
It has an unusual humeral insertion in that the clavicular and upper sternal fibres spiral to attach distally on the humerus,
while the lower sternal and abdominal fibres cross above the former and insert uppermost on the shaft of the humerus.
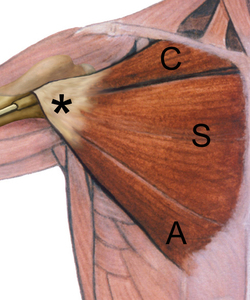
Fig. 9: Illustration of normal pectoralis major anatomy, showing the clavicular (C), sternal (S) and abdominal (A) heads converging to form a single trilaminar tendon (asterisk). Reproduced with permission from Ref 19.
Tears to the pectoralis muscle have been reported following a direct blow14 but typically injuries occur indirectly during eccentric muscular contraction15,16.
High-grade injury occurs predominantly in male athletes participating in weight lifting,
waterskiing,
and contact sports such as American football,
rugby,
or wrestling17 where the muscle under full tension and is then subjected to acute stress.
The most often cited mechanism of injury is in weightlifters performing the bench-press maneuver18.
Non-sports injuries have been reported; in this group the most common mechanism of injury was forced abduction with extension and/or external rotation during a fall or while lifting19.
Interestingly,
tears due to non-sports injuries,
both complete and partial,
predominate at the musculotendinous junction.
In comparison,
most sports-related complete tears occur at the insertion,
whereas partial tears in this group of patients typically involve the musculotendinous junction20,21.
It should be considered that most mild strains and partial tears likely go unreported22.
Tears of the muscle belly,
in contrast,
are most commonly seen associated with direct trauma from crush injuries and road traffic accidents23.
Clinically,
there is sudden pain in the arm or shoulder that may be accompanied by an audible pop and swelling with ecchymosis.
It may be possible to palpate a defect,
and on inspection loss of the anterior axillary fold and/or asymmetry on comparison with the other side may be apparent.
Loss of strength in adduction is often subtle but becomes important in athletes such as weight lifters.
The cosmetic abnormality may also be of consequence,
for example in body builders,
and may influence management decisions.
Differentiation between injury to the musculotendinous junction and avulsion at the humeral attachment has a significant bearing on management,
with the former generally responding well to conservative treatment while humeral avulsion typically requires surgical repair17,19.20,22. Clinical assessment can be hampered by muscle spasm and hematoma,
and so accurate diagnostic imaging is essential.
A significant proportion of patients are initially misdiagnosed or present late; a consideration when interpreting imaging findings.
Tears are described by location (i.e.,
at the origin,
muscle belly,
musculotendinous junction,
or insertion).
Grading,
as in other muscle groups,
can be divided into grades 1 to 3; however,
subdividing pectoralis major injuries into complete or incomplete in relation to the clavicular and sternal heads is generally more clinically useful.
Imaging
Plain radiographs can sometimes be helpful in checking for humeral avulsion fractures.
Soft tissue swelling or an absent pectoralis major shadow may also be seen. US is very useful and has been shown to correlate well with MR imaging and operative findings (Fig. 10, Fig. 11,
Fig. 12,
Fig. 13,
Fig. 10, Fig. 14). Static and dynamic assessment is performed with the arm in abduction and external rotation (ABER).
This adds stress to the musculotendinous junction,
which is the most common site of partial rupture and the amount of retraction can be measured. A systematic review of each of the three heads,
which blend laterally before insertion onto the humerus,
is advocated.
Imaging longitudinally along the fibres may show disruption,
retraction and haematoma,
most commonly involving the musculotendinous junction of the sternal head24, (Fig. 15).
Gentle dynamic assessment will help differentiate haematoma and debris from intact muscle.
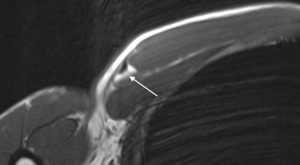
Fig. 10: Rugby league player with a history of previous pectoralis muscle tear and suspected re-injury. Axial T1w MR image shows some fatty change (arrow) distally around the musculotendinous junction suggestive of previous injury.
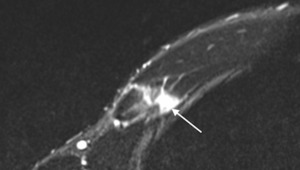
Fig. 11: Rugby league player with a history of previous pectoralis muscle tear and suspected re-injury. Axial T2w fat suppressed MR image shows features consistent with an acute tear of the costal attachment of the deep pectoralis major (arrows). There is oedema and muscle disruption but the more superior fibres of the deep component remain intact (Grade II injury).
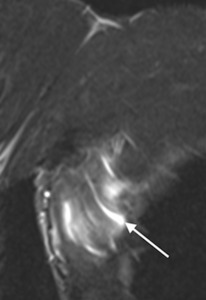
Fig. 12: Rugby league player with a history of previous pectoralis muscle tear and suspected re-injury. Coronal T2w fat suppressed MR image shows features consistent with an acute tear of the costal attachment of the deep pectoralis major (arrows). There is oedema and muscle disruption but the more superior fibres of the deep component remain intact (Grade II injury).
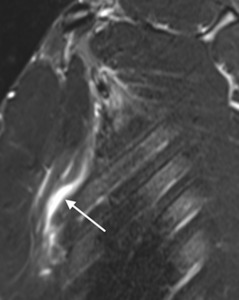
Fig. 13: Rugby league player with a history of previous pectoralis muscle tear and suspected re-injury. Sagittal T2w fat suppressed MR image shows features consistent with an acute tear of the costal attachment of the deep pectoralis major (arrows). There is oedema and muscle disruption but the more superior fibres of the deep component remain intact (Grade II injury).
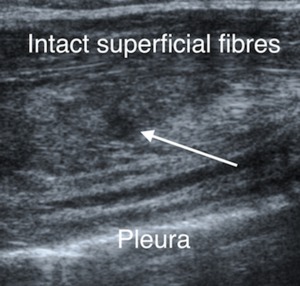
Fig. 14: Rugby league player with a history of previous pectoralis muscle tear and suspected re-injury. Ultrasound image shows the tear and haematoma involving the deep costal attachment (arrow).
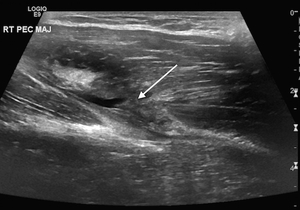
Fig. 15: Rugby league player with right sided chest pain and arm weakness after bench pressing. Axial ultrasound image shows a partial thickness tear at the musculotendinous junction of the sternal head of pectoralis major (arrow).
MR imaging is better described in the literature and has been shown to be more sensitive to low grade strains and tears.
It provides greater anatomical detail and has been shown to correlate very well with surgical findings25. Ideally,
a dedicated surface coil with a unilateral field of view and thin 3-4 mm sections are acquired20 with the arm in the ABER position.
Most patients however will not be able to tolerate this position for the required length of time and the arm is usually best left in the neutral position. In the sports patient with large muscles a wide bore scanner may be required for optimum positioning. Standard sequences in axial and coronal oblique planes along the axis of the tendon are acquired.
Low-grade partial tears are most commonly seen within the muscle belly or at the musculotendinous junction,
unlike avulsions and complete tears.
Haematoma and oedema are indicators of an acute injury (Fig. 16, Fig. 17,
Fig. 18,
Fig. 19 Fig. 20,
Fig. 21,
Fig. 22,
Fig. 23).
The amount of retraction of torn fibres is highly variable but may be minimal if remnants of the clavicular head remain intact or when the investing fascia of the muscle remains continuous with fascia of the brachium and the medial antebrachial septum26. If the tendon is avulsed from its humeral insertion however,
periosteal stripping may be seen as focal T2 hyperintensity immediately superficial to the humeral cortex. The hypointense tendon end should always be looked for along the lateral margin of the tubercular groove,
usually at 1 – 1.5 cm inferior to the quadrilateral space and 1 cm superior to the origin of the lateral head of the triceps muscle27.
A good secondary sign however is the finding of T2 hyperintense fluid signal at the leading edge of the muscle and surrounding the biceps tendon in the bicipital groove27.
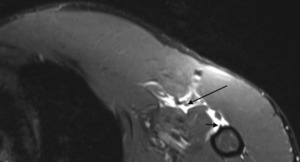
Fig. 16: Rugby league player with complete pectoralis major tendon tear at the humeral shaft insertion following a fall on outstretched arm. Axial T2w fat suppressed MR image confirms tendon rupture with retraction of the musculotendinous junction of approximately 4.3 cm (long arrow). There is a small remnant of tendon protruding from the humeral shaft (short arrow) with no bone marrow oedema to suggest periosteal stripping.
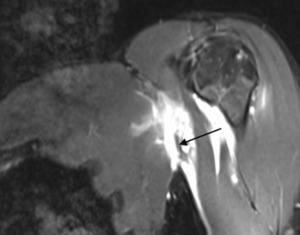
Fig. 17: Rugby league player with complete pectoralis major tendon tear at the humeral shaft insertion following a fall on outstretched arm. Coronal T2w fat suppressed MR image confirms tendon rupture with retraction of the musculotendinous junction of approximately 4.3 cm (long arrow). There is a small remnant of tendon protruding from the humeral shaft (short arrow) with no bone marrow oedema to suggest periosteal stripping.
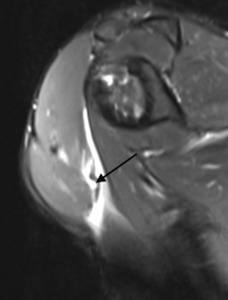
Fig. 18: Rugby league player with complete pectoralis major tendon tear at the humeral shaft insertion following a fall on outstretched arm. Sagittal T2w fat suppressed MR image confirms tendon rupture with retraction of the musculotendinous junction of approximately 4.3 cm (long arrow). There is a small remnant of tendon protruding from the humeral shaft (short arrow) with no bone marrow oedema to suggest periosteal stripping.
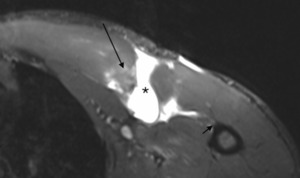
Fig. 19: Rugby league player with a left pectoralis major muscle tear. Axial T2w fat supressed MR image shows a complete tear at the musculotendinous junction of the sternal head. At the site of the tear there is a large volume of liquefied haematoma (asterisk). The more proximal muscle shows residual oedema (long arrow). Distal to the haematoma there is an intact tendon remnant insertion into the humeral shaft (short arrow).
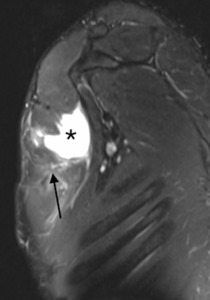
Fig. 20: Rugby league player with a left pectoralis major muscle tear. Coronal T2w fat supressed MR image shows a complete tear at the musculotendinous junction of the sternal head. At the site of the tear there is a large volume of liquefied haematoma (asterisk). The more proximal muscle shows residual oedema (long arrow). Distal to the haematoma there is an intact tendon remnant insertion into the humeral shaft (short arrow).
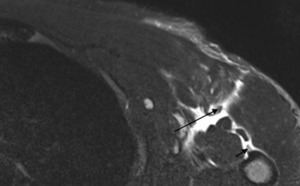
Fig. 21: Rugby union player with a grade III musculotendinous injury of pectoralis major. Axial T2w fat supressed MR image shows retraction of the tendon (long arrow) into the oedematous muscle and a small tendon remnant at the humeral insertion (short arrow). There is a large volume of fluid and haematoma in between. The injury involved the abdominal and sternal head with no significant involvement of the clavicular head.
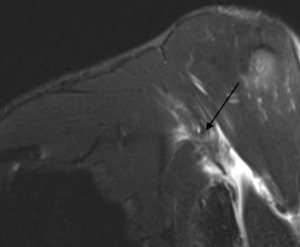
Fig. 22: Rugby union player with a grade III musculotendinous injury of pectoralis major. Coronal T2w fat supressed MR image shows retraction of the tendon (long arrow) into the oedematous muscle and a small tendon remnant at the humeral insertion (short arrow). There is a large volume of fluid and haematoma in between. The injury involved the abdominal and sternal head with no significant involvement of the clavicular head.
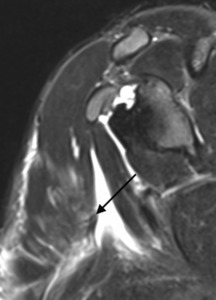
Fig. 23: Rugby union player with a grade III musculotendinous injury of pectoralis major. Sagittal T2w fat supressed MR image shows retraction of the tendon (long arrow) into the oedematous muscle and a small tendon remnant at the humeral insertion (short arrow). There is a large volume of fluid and haematoma in between. The injury involved the abdominal and sternal head with no significant involvement of the clavicular head.
In chronic cases the degree of fibrotic change and fatty atrophy are well appreciated on T1 images,
(Fig. 24, Fig. 25).
MR is useful for injury follow-up although there is no data in the literature on the ability of MRI to predict recovery time and return to sport26.
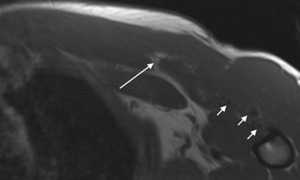
Fig. 24: Same patient as Figs 20 - 22, six months after injury and following surgical repair. Axial T1w image shows surgical artefact along the musculotendinous region and around the anterior humerus consistent with tendon reattachment and tunnelling (short arrows). There is fat atrophy (long arrows) within the abdominal and sternal heads of pectoralis major.
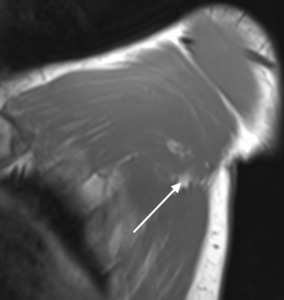
Fig. 25: Same patient as Figs 20 - 23, six months after injury and following surgical repair. Coronal T1w image shows fat atrophy (long arrows) within the abdominal and sternal heads of pectoralis major.
Pectoralis Minor
Isolated pectoralis minor tears are unusual and have rarely been reported in the literature.
The pectoralis minor muscle originates between the anterior 2nd to 5th ribs and inserts onto the coracoid process adjacent to the conjoint tendon.
As with pectoralis major,
US is useful for targeted evaluation but MRI is usually required for a better anatomical overview (Fig. 26,
Fig. 27,
Fig. 28, Fig. 29)
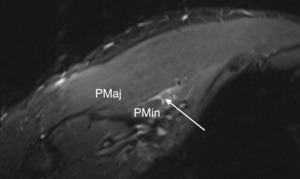
Fig. 26: Rugby union player with an isolated pectoralis minor rupture. High axial T2w fat supressed MR image shows high signal haematoma near the muscle origin between the 2nd and 5th ribs (long arrow). PMaj, pectoralis major; PMin, pectoralis minor.
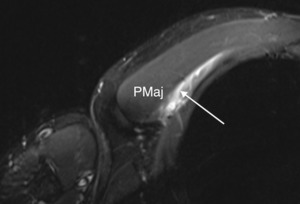
Fig. 27: Rugby union player with an isolated pectoralis minor rupture. Low axial T2w fat supressed MR image shows high signal haematoma near the muscle origin between the 2nd and 5th ribs (long arrow). PMaj, pectoralis major.
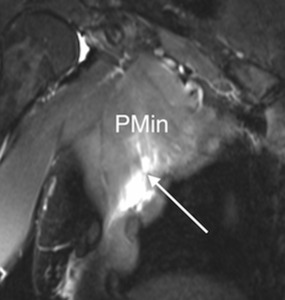
Fig. 28: Rugby union player with an isolated pectoralis minor rupture. Coronal T2w fat supressed MR image shows high signal haematoma near the muscle origin between the 2nd and 5th ribs (long arrow). PMin, pectoralis minor.
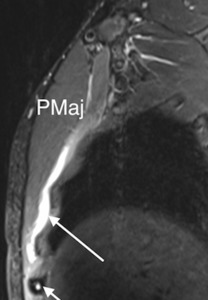
Fig. 29: Rugby union player with an isolated pectoralis minor rupture. Sagittal T2w fat supressed MR image shows high signal haematoma near the muscle origin between the 2nd and 5th ribs (long arrow). High signal marrow oedema is seen in the anterior 5th rib (sagittal image; short arrow) secondary to recent local trauma. PMaj, pectoralis major.
Side strain
Side strain is a term that describes a tear to the internal oblique muscle,
or less commonly the external oblique,
at the superior attachment onto the ninth to twelfth ribs,
costal cartilage and intercostal muscles7.
The internal oblique muscle contains a higher percentage of type II muscle fibres,
which may be a predisposition to injury.
The mechanism of injury is a sudden eccentric contraction,
as seen in the non-bowling arm of pace bowlers in cricket during the final delivery action,
when the non-bowling arm is forcefully pulled down with the trunk in lateral flexion28,29.
A similar mechanism is described in baseball pitchers during the late cocking and early acceleration stages of throwing when the non-dominant arm is suddenly pulled down with the trunk hyperextended27. Rowers and swimmers are susceptible due to strong rotation forces associated with forced contraction of rectus abdominis.
Clinical presentation occurs with acute pain and tenderness over the lower four ribs and costal cartilages that can be exacerbated by resisted lateral flexion to the affected side29. There is a high proportion of recurrent injury28.
Imaging
Although the diagnosis is generally a clinical one,
imaging can assist in evaluation of injury severity to help guide rehabilitation.
US assessment of side strain will show loss of normal architecture and a hypoechoic gap at the insertion of internal oblique onto the costal cartilage and rib26 (Fig. 30).
Fiber retraction however is usually minimal given the broad origin of the muscle.
Hematoma can be seen at the injury site,
especially if there is osseous or chondral cartilage avulsion and stripping of the periosteum,
and fluid may be traced between the muscle layers.
Associated bone injury is typically better evaluated at MRI,
but bone avulsion can be seen29. US is less sensitive when the injury is not acute and/or the muscle tear is small29.
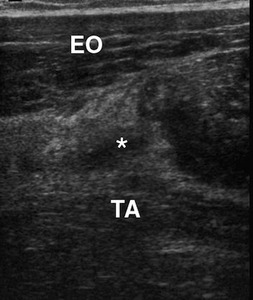
Fig. 30: Rugby league player with a side strain following an isolated twisting injury. Axial ultrasound image of the right lateral chest wall shows focal hypoechogenicity at the site of an internal oblique muscle tear (asterisk). EO, external oblique; TA, transversalis abdominis.
MR imaging is complicated by respiration movement artifact but has been shown to be of use in injury assessment.
The patient is best scanned using a 3 Tesla magnet with it’s relatively wide bore.
A skin marker is used to localize the area of concern and a flexible surface coil used to obtain a large FOV sequence in order to count the underlying ribs.
Sagittal oblique T1-weighted thin slices are then obtained with a small FOV through the area of concern (Fig. 31 ,
Fig. 32 ,
Fig. 33). Positive findings include haematoma at the injury site,
periosteal stripping,
and chronic stress injury to the underlying rib1,30 (Fig. 34).
MR is especially useful in the assessment of concomitant injury to the external oblique muscle acutely31,
and more long term it can be used in follow-up of patients who fail to respond to conservative measures,
( Fig. 35,
Fig. 36,
Fig. 37).
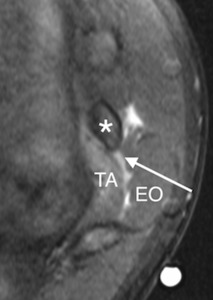
Fig. 31: Cricket player (right arm bowler) with a side strain injury to the left internal oblique. Axial T2w fat supressed MR images show a grade II tear (arrow) to the costal attachment of internal oblique (IO). Adjacent are the intact transversalis abdominis (TA) and external oblique (EO) muscles and 11th rib (asterisk).
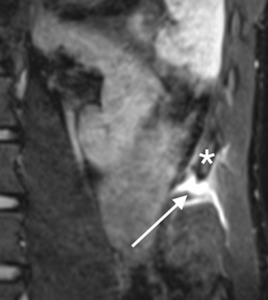
Fig. 32: Cricket player (right arm bowler) with a side strain injury to the left internal oblique. Coronal (large field of view) T2w fat supressed MR image shows a grade II tear. Adjacent is the intact 11th rib (asterisk).
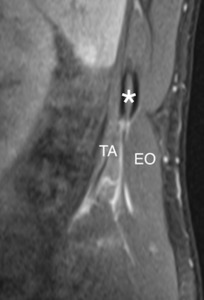
Fig. 33: Cricket player (right arm bowler) with a side strain injury to the left internal oblique. Coronal oblique (small field of view) T2w fat supressed MR image shows a grade II tear to the costal attachment of internal oblique. Adjacent are the intact transversalis abdominis (TA) and external oblique (EO) muscles and 11th rib (asterisk).
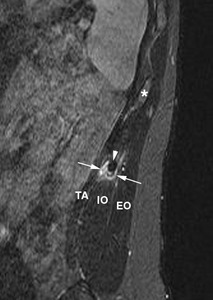
Fig. 34: A different cricket player and right arm bowler with a left side strain injury to internal oblique. Coronal oblique T2w fat-suppressed image of the chest wall with a tear (arrows) in the internal oblique (IO) between transversalis abdominis (TA) and external oblique (EO). The adjacent 11th rib is hypertrophied due to chronic stress (arrow-head); compare with normal rib (asterisk). Reproduced with permission from Ref 30.
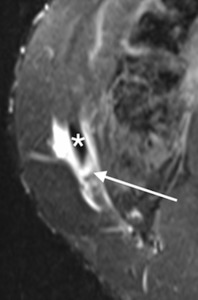
Fig. 35: Soccer player with a right internal oblique strain following a twisting movement. Axial T2w fat supressed MR image shows a grade II internal oblique (IO) tear at its attachment to the lower right 11th rib (asterisk) with adjacent haematoma (arrows). There is no evidence of bone marrow oedema within the rib to suggest more significant disruption. The external oblique and transverse abdominis muscles are intact.
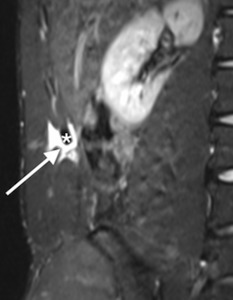
Fig. 36: Soccer player with a right internal oblique strain following a twisting movement. Coronal with large field of view T2w fat supressed MR image shows a grade II internal oblique tear at its attachment to the lower right 11th rib (asterisk) with adjacent haematoma (arrow). There is no evidence of bone marrow oedema within the rib to suggest more significant disruption. The external oblique and transverse abdominis muscles are intact.
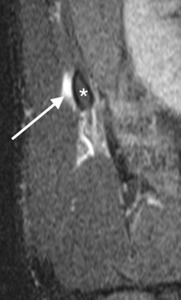
Fig. 37: Soccer player with a right internal oblique strain following a twisting movement. Coronal oblique with small field of view T2w fat supressed MR image shows a grade II internal oblique tear at its attachment to the lower right 11th rib (asterisk) with adjacent haematoma (arrow). There is no evidence of bone marrow oedema within the rib to suggest more significant disruption. The external oblique and transverse abdominis muscles are intact.
Shoulder and upper arm
Rotator cuff tears are common injuries in athletes and usually result from repetitive overhead activity such as throwing in javelin,
tennis or baseball.
Throwing velocity is related to increased range of movement in shoulder abduction and external rotation.
Training to increase this range can lead to a contracture in the posterior capsule and subsequent posterosuperior humeral head migration,
known as glenohumeral internal rotation defecit (GIRD).
The associated osseous impingement can lead to posterosuperior rotator cuff tears and labral damage32.
Throwing athletes are therefore prone to articular-sided partial-thickness tears to the posterior fibres of supraspinatus tendon35.
Imaging of the rotator cuff is beyond the scope of this chapter but for the throwing athlete,
MR arthrography is considered the gold standard due to its ability to outline an articular sided tear as well as any associated labral damage and posterior capsular thickening.
Direct muscle belly injuries around the shoulder are commonly due to blunt impact during contact sports such as rugby.
This typically results in a contusion,
however in patients with an underlying bleeding disorder,
seemingly insignificant trauma can result in extensive intramuscular haemorrhage with risk of compartment syndrome.
Joint dislocation can also cause muscle fibre damage,
which may not be appreciated on presentation. Upper limb lacerations are rare but often underestimated.
Indirect muscle injuries usually involve the musculotendinous junction in young athletes (Fig. 38,
Fig. 39) and the tendon at its osseous insertion in the elderly.
In any age group,
isolated muscle belly injuries are rare (Fig. 40 ,
Fig. 41,
Fig. 42).
At the shoulder the long head of biceps tendon may rupture due to indirect eccentric loading causing pain and deformity.
Although often obvious clinically,
US and MR imaging have been shown to provide valuable additional information33-36.
Care must be taken to correctly diagnose muscle belly tears.
The rarity of such injuries in the upper extremity may predispose to misdiagnosis as mores sinister pathology such as malignancy36.
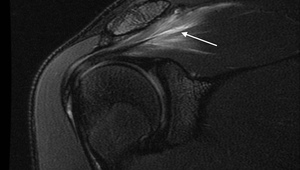
Fig. 38: Young Olympic sprint athlete with shoulder pain. Coronal PD fat supressed MR image showing a grade 2 musculotendinous strain of the supraspinatus muscle (arrow).
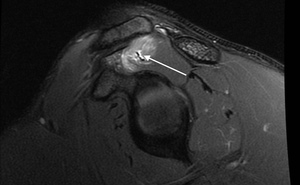
Fig. 39: Young Olympic sprint athlete with shoulder pain. Sagittal PD fat supressed MR image showing a grade 2 musculotendinous strain of the supraspinatus muscle (arrow).
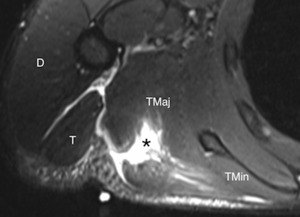
Fig. 40: Young cricket player (right sided bowler) presented with a grade II tear of right teres major muscle (TM). Axial T2w fat supressed MR image shows a tear involving the superficial muscle fibres involving 80% of the muscle at its maximum depth (asterisk). The deep portion of the muscle is intact. Fluid is interposed between the muscle fibres, and oedema extends into the muscle belly to both sides of the tear. TMaj, teres major; TMin, teres minor; T, triceps; D, deltoid; ISP, infraspinatus.
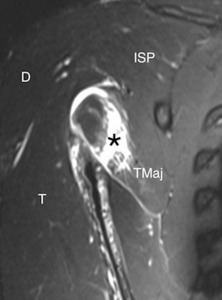
Fig. 41: Young cricket player (right sided bowler) presented with a grade II tear of right teres major muscle (TM). Coronal T2w fat supressed MR image shows a tear involving the superficial muscle fibres involving 80% of the muscle at its maximum depth (asterisk). The deep portion of the muscle is intact. Fluid is interposed between the muscle fibres, and oedema extends into the muscle belly to both sides of the tear. TMaj, teres major; TMin, teres minor; T, triceps; D, deltoid; ISP, infraspinatus.
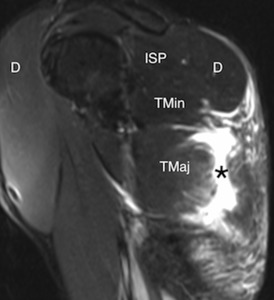
Fig. 42: Young cricket player (right sided bowler) presented with a grade II tear of right teres major muscle (TM). Sagittal T2w fat supressed MR image shows a tear involving the superficial muscle fibres involving 80% of the muscle at its maximum depth (asterisk). The deep portion of the muscle is intact. Fluid is interposed between the muscle fibres, and oedema extends into the muscle belly to both sides of the tear. TMaj, teres major; TMin, teres minor; T, triceps; D, deltoid; ISP, infraspinatus.
The largest series of indirect muscle injury of the biceps brachii is reported in military static line parachuting where the static line becomes wrapped around the upper arm causing forced arm abduction and transection of the muscle belly37 (Fig. 43).
More recently,
rupture of the proximal muscle belly has also been described in wakeboarders,
water skiers,
and other water sports utilising a towline38,
where the short and long heads may be stripped down to the forearm by the handle.
Early diagnosis of the muscle rupture is critical as early operative repair leads to good functional and cosmetic results.
Associated symptoms from the musculocutaneous nerve have been described following biceps brachii tears,
perhaps not surprising given the close proximity of the nerve.
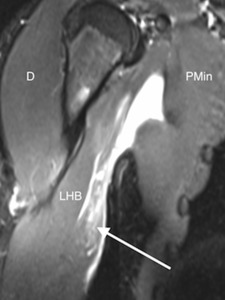
Fig. 43: Rugby league player with sudden arm pain and weakness following a tackle. Coronal T2w fat suppressed MR image shows abnormal signal in the proximal musculotendinous junction of the short head of bicep’s brachii (arrow). This is associated with extensive haemorrhage in the interfascial planes. The tear itself measures around 8 cm in length with architectural distortion and some retraction of muscle fibres in keeping with a grade II injury. The long head of biceps, deltoid and pectoralis minor image normally although are surrounded by fluid/haemorrhage. LHB, long head of biceps; D, deltoid; PMin, pectoralis minor.
Elbow and lower arm
Injuries to the distal biceps tendon are much less common than injuries of the proximal tendon.
Most distal biceps tears are seen in middle-aged men during weightlifting.
Other risk factors include anabolic steroids,
and smoking39. Clinical presentation classically relates to a painful “pop” followed by swelling and ecchymosis in the antecubital fossa with a distinct asymmetry in biceps muscle contour and a non-palpable distal tendon.
There may be clinical confusion however if the lacertus fibrosis (bicipital aponeurosis) remains intact as this may prevent retraction of the torn tendon and limit ecchymosis formation.
US can help differentiate tendinosis from a complete tear in the acute setting by assessing tendon diameter,
echogenicity and the degree of retraction.
Partial or chronic tears may require MR imaging.
The presence of T2 hyperintensity within an abnormally thickened or thinned tendon may indicate a partial tear or advanced tendinopathy40. Bone marrow can also be assessed for oedema as an indicator of avulsion.
The elbow is best imaged lying prone with the arm overhead in the so-called “superman” position.
The elbow is then flexed to 90 degrees and the forearm supinated. This flexed abducted supinated position (FABS) helps to stretch the tendon but may be uncomfortable for the patient36 (Fig. 44).

Fig. 44: Photograph showing the Flexed Abducted Supinated Position (FABS) of the elbow with an MRI coil used to image the distal biceps tendon.
Isolated brachialis muscle tears are extremely rare with only three reported cases in the literature36,41. Brachialis is a powerful elbow flexor in the pronated forearm and is important in climbing with strain injuries known as “climber’s elbow”42,
(Fig. 45, Fig. 46).

Fig. 45: Rugby league player with strain injury of brachialis muscle. The patient had a slight fixed flexion deformity of the elbow following a match. Sagittal T2w fat suppressed MR image shows abnormal high signal (arrow) at the distal musculotendinous junction.
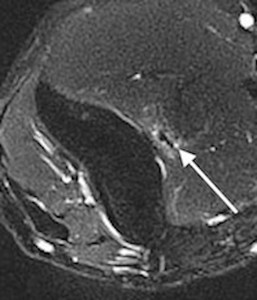
Fig. 46: Rugby league player with strain injury of brachialis muscle. The patient had a slight fixed flexion deformity of the elbow following a match. Axial T2w fat suppressed MR image shows abnormal high signal (arrow) at the distal musculotendinous junction.
Flexor-pronator tendinosis or rupture is seen in overhead throwing sports,
racquet sports or golf,
resulting in a chronic valgus overuse injury (Fig. 8).
It is more common in athletes than non-athletes.
Baseball pitchers get strains either as an isolated injury or in elbow valgus instability with ulnar collateral ligament disruption41. Strains or tears to the muscle belly are less common than to the tendon origin but can be recognised on MRI by fluid signal extending into the muscle bellies of the flexor tendons (Fig. 47,
Fig. 48,
Fig. 49,
Fig. 50).
Likewise,
extensor-supinator injuries seen at the common extensor origin as ‘tennis elbow’ may extend into the muscle belly as a muscular strain or partial tear.
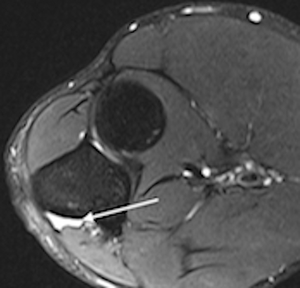
Fig. 47: Policeman with elbow pain and a previous tear at the origin of flexor digitorum profundus (FDP). Axial T2w fat suppressed MR image shows a seroma between the muscle and bone at the FDP origin (arrow). There is no evidence of oedema within the muscle, surrounding soft tissues or the adjacent ulna to imply recent damage.
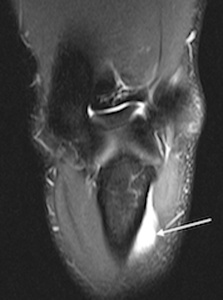
Fig. 48: Policeman with elbow pain and a previous tear at the origin of flexor digitorum profundus (FDP). Coronal T2w fat suppressed MR image shows a seroma between the muscle and bone at the FDP origin (arrow). There is no evidence of oedema within the muscle, surrounding soft tissues or the adjacent ulna to imply recent damage.
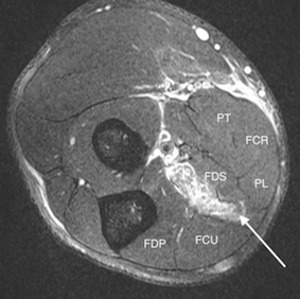
Fig. 49: Rugby player with a grade 2 strain injury of flexor digitorum superficialis (FDS) following a hyperextension injury during training. Axial T2w fat suppressed MR images show high signal (arrow) at the proximal musculotendinous junction of FDS. There is fluid within the muscle belly distally and fluid/haemorrhage tracking along the fascial planes. FDS, flexor digitorum superficialis; FDP, flexor digitorum profundus; FCU, flexor carpi ulnaris; PL, palmaris longus; FCR, flexor carpi radialis; PT, pronator teres.
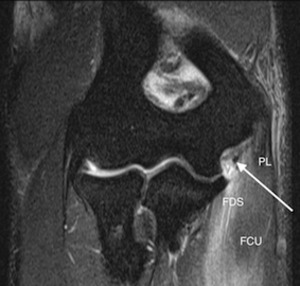
Fig. 50: Rugby player with a grade 2 strain injury of flexor digitorum superficialis (FDS) following a hyperextension injury during training. Coronal T2w fat suppressed MR images show high signal (arrow) at the proximal musculotendinous junction of FDS. There is fluid within the muscle belly distally and fluid/haemorrhage tracking along the fascial planes. FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris; PL, palmaris longus;
Triceps brachii muscle ruptures are extremely rare but have been reported to result from a fall onto an outstretched hand,
from direct trauma or from forced elbow flexion with eccentric failure42.
Radiographs may show soft tissue swelling with a possible avulsion fracture from the olecranon.
US and MR imaging is used to assess the tendon for partial or complete rupture and to check the muscle belly for evidence of a strain or haematoma (Fig. 51).
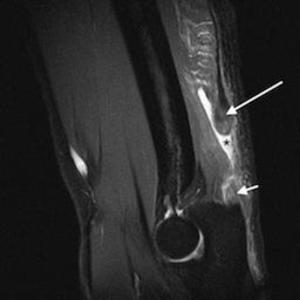
Fig. 51: Rugby player with complete rupture of the triceps at the distal musculotendinous junction (long arrow). Sagittal T2w fat suppressed MR image shows haematoma (asterisk) surrounding the tear and retraction by about 4 cm. There is oedema in the retracted muscle belly. A small remnant of tendon remains at the olecranon insertion (short arrow).


 spreading across the lumbrical muscles on the palmar aspect of the hand.")
 Radiograph shows a soft tissue mass (asterisk) with classical peripheral calcification (arrows).")
 with posterior acoustic shadowing and normal surrounding tissue planes.")
 with peripheral low signal calcification (arrows) and marked surrounding oedema.")
 with peripheral low signal calcification (arrows) and marked surrounding oedema.")
.")
, sternal (S) and abdominal (A) heads converging to form a single trilaminar tendon (asterisk). Reproduced with permission from Ref 19.")
. There is oedema and muscle disruption but the more superior fibres of the deep component remain intact (Grade II injury).")
. There is oedema and muscle disruption but the more superior fibres of the deep component remain intact (Grade II injury).")
. There is oedema and muscle disruption but the more superior fibres of the deep component remain intact (Grade II injury).")
 distally around the musculotendinous junction suggestive of previous injury.")
.")
.")
. There is a small remnant of tendon protruding from the humeral shaft (short arrow) with no bone marrow oedema to suggest periosteal stripping.")
. There is a small remnant of tendon protruding from the humeral shaft (short arrow) with no bone marrow oedema to suggest periosteal stripping.")
. There is a small remnant of tendon protruding from the humeral shaft (short arrow) with no bone marrow oedema to suggest periosteal stripping.")
. The more proximal muscle shows residual oedema (long arrow). Distal to the haematoma there is an intact tendon remnant insertion into the humeral shaft (short arrow).")
. The more proximal muscle shows residual oedema (long arrow). Distal to the haematoma there is an intact tendon remnant insertion into the humeral shaft (short arrow).")
 into the oedematous muscle and a small tendon remnant at the humeral insertion (short arrow). There is a large volume of fluid and haematoma in between. The injury involved the abdominal and sternal head with no significant involvement of the clavicular head.")
 into the oedematous muscle and a small tendon remnant at the humeral insertion (short arrow). There is a large volume of fluid and haematoma in between. The injury involved the abdominal and sternal head with no significant involvement of the clavicular head.")
 into the oedematous muscle and a small tendon remnant at the humeral insertion (short arrow). There is a large volume of fluid and haematoma in between. The injury involved the abdominal and sternal head with no significant involvement of the clavicular head.")
. There is fat atrophy (long arrows) within the abdominal and sternal heads of pectoralis major.")
 within the abdominal and sternal heads of pectoralis major.")
. PMaj, pectoralis major; PMin, pectoralis minor.")
. PMaj, pectoralis major.")
. PMin, pectoralis minor.")
. High signal marrow oedema is seen in the anterior 5th rib (sagittal image; short arrow) secondary to recent local trauma. PMaj, pectoralis major.")
. EO, external oblique; TA, transversalis abdominis.")
 with a side strain injury to the left internal oblique. Axial T2w fat supressed MR images show a grade II tear (arrow) to the costal attachment of internal oblique (IO). Adjacent are the intact transversalis abdominis (TA) and external oblique (EO) muscles and 11th rib (asterisk).")
 with a side strain injury to the left internal oblique. Coronal (large field of view) T2w fat supressed MR image shows a grade II tear. Adjacent is the intact 11th rib (asterisk).")
 with a side strain injury to the left internal oblique. Coronal oblique (small field of view) T2w fat supressed MR image shows a grade II tear to the costal attachment of internal oblique. Adjacent are the intact transversalis abdominis (TA) and external oblique (EO) muscles and 11th rib (asterisk).")
.")
.")
 presented with a grade II tear of right teres major muscle (TM). Axial T2w fat supressed MR image shows a tear involving the superficial muscle fibres involving 80% of the muscle at its maximum depth (asterisk). The deep portion of the muscle is intact. Fluid is interposed between the muscle fibres, and oedema extends into the muscle belly to both sides of the tear. TMaj, teres major; TMin, teres minor; T, triceps; D, deltoid; ISP, infraspinatus.")
 presented with a grade II tear of right teres major muscle (TM). Coronal T2w fat supressed MR image shows a tear involving the superficial muscle fibres involving 80% of the muscle at its maximum depth (asterisk). The deep portion of the muscle is intact. Fluid is interposed between the muscle fibres, and oedema extends into the muscle belly to both sides of the tear. TMaj, teres major; TMin, teres minor; T, triceps; D, deltoid; ISP, infraspinatus.")
 presented with a grade II tear of right teres major muscle (TM). Sagittal T2w fat supressed MR image shows a tear involving the superficial muscle fibres involving 80% of the muscle at its maximum depth (asterisk). The deep portion of the muscle is intact. Fluid is interposed between the muscle fibres, and oedema extends into the muscle belly to both sides of the tear. TMaj, teres major; TMin, teres minor; T, triceps; D, deltoid; ISP, infraspinatus.")
. This is associated with extensive haemorrhage in the interfascial planes. The tear itself measures around 8 cm in length with architectural distortion and some retraction of muscle fibres in keeping with a grade II injury. The long head of biceps, deltoid and pectoralis minor image normally although are surrounded by fluid/haemorrhage. LHB, long head of biceps; D, deltoid; PMin, pectoralis minor.")
 of the elbow with an MRI coil used to image the distal biceps tendon.")
 at the distal musculotendinous junction.")
 following a hyperextension injury during training. Axial T2w fat suppressed MR images show high signal (arrow) at the proximal musculotendinous junction of FDS. There is fluid within the muscle belly distally and fluid/haemorrhage tracking along the fascial planes. FDS, flexor digitorum superficialis; FDP, flexor digitorum profundus; FCU, flexor carpi ulnaris; PL, palmaris longus; FCR, flexor carpi radialis; PT, pronator teres.")
 following a hyperextension injury during training. Coronal T2w fat suppressed MR images show high signal (arrow) at the proximal musculotendinous junction of FDS. There is fluid within the muscle belly distally and fluid/haemorrhage tracking along the fascial planes. FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris; PL, palmaris longus;")
. Sagittal T2w fat suppressed MR image shows haematoma (asterisk) surrounding the tear and retraction by about 4 cm. There is oedema in the retracted muscle belly. A small remnant of tendon remains at the olecranon insertion (short arrow).")
 in the internal oblique (IO) between transversalis abdominis (TA) and external oblique (EO). The adjacent 11th rib is hypertrophied due to chronic stress (arrow-head); compare with normal rib (asterisk). Reproduced with permission from Ref 30.")
 tear at its attachment to the lower right 11th rib (asterisk) with adjacent haematoma (arrows). There is no evidence of bone marrow oedema within the rib to suggest more significant disruption. The external oblique and transverse abdominis muscles are intact.")
 with adjacent haematoma (arrow). There is no evidence of bone marrow oedema within the rib to suggest more significant disruption. The external oblique and transverse abdominis muscles are intact.")
 with adjacent haematoma (arrow). There is no evidence of bone marrow oedema within the rib to suggest more significant disruption. The external oblique and transverse abdominis muscles are intact.")
 at the distal musculotendinous junction.")
. Axial T2w fat suppressed MR image shows a seroma between the muscle and bone at the FDP origin (arrow). There is no evidence of oedema within the muscle, surrounding soft tissues or the adjacent ulna to imply recent damage.")
. Coronal T2w fat suppressed MR image shows a seroma between the muscle and bone at the FDP origin (arrow). There is no evidence of oedema within the muscle, surrounding soft tissues or the adjacent ulna to imply recent damage.")
