Accessory and sesamoid bones are normal structures of the foot that in normal conditions are asymptomatic.
They are generally small,
well-corticated and ovoid bones.
Sesamoid bones may be bipartite or multipartite,
and are located close to a bone or a joint.
Awareness of the presence of sesamoids and accessory bones is helpful to not misdiagnose them as fractures.
Although rare,
symptomatic accessory and sesamoid bones may be associated with painful syndromes,
due to various pathologies,
including trauma,
infection,
inflammation and degeneration.
Sesamoid Bones
Sesamoids are osseous structures partially or totally embedded in a tendon and their function is to protect the tendon from injury by reducing friction.
Normal anatomy and appearance
There are three types of sesamoids: the hallucal sesamoids (most common and always present),
the lesser metatarsal sesamoids and the interphalangeal joint sesamoid.
The hallux sesamoids locate at the plantar aspect of the first metatarsal head.
They are commonly two and the medial one frequently demonstrate bipartite variation.
It is crucial to recognize this variation since it can be mistakenly recognized as a fracture.

Fig. 2: Anteroposterior and oblique views of the foot showing hallux sesamoids
References: Department of Radiology, Hospital de São João, Porto, Portugal
The lesser metatarsal sesamoids locate at the plantar aspect of the second through fifth metatarsals and appear to be embedded in the joint capsule.
They can also be multiple or multipartite.

Fig. 3: Anteroposterior and oblique views of the foot showing a lesser fifth metatarsal sesamoid.
References: Department of Radiology, Hospital de São João, Porto, Portugal

Fig. 4: Anteroposterior radiograph of the foot showing lesser metatarsal sesamoids in a patient with a stress fracture (2nd metatarsal bone)
References: Department of Radiology, Hospital de São João, Porto, Portugal
The interphalangeal joint sesamoid locates at the plantar aspect of the interphalangeal joint of the first digit of the foot.
It is embedded within the joint capsule and its presence can limit motion of this joint.
Pathologic conditions
Bipartite Hallux Sesamoid
The hallux sesamoid bones develop from two ossification centers and they do not fuse at maturity,
forming a bipartite sesamoid bone.
The medial hallux sesamoid tends to be bipartite in morphology.
This anatomical aspect is important once it should be differentiated from a sesamoid fracture.
A true sesamoid bone fracture usually demonstrates a fragment that is not oval in shape and that don’t have well corticated margins and the patient complains of an acute onset of pain and tenderness on direct palpation over the injured sesamoid bone.

Fig. 5: Anteroposterior and oblique views of the foot showing hallux sesamoids with the medial one demonstrating bipartite variation
References: Department of Radiology, Hospital de São João, Porto, Portugal

Fig. 6: MRI. T1, Axial; Medial bipartite sesamoid
References: Department of Radiology, Hospital de São João, Porto, Portugal
Sesamoid bones syndrome
Sesamoid bones syndrome refers to the deformation,
cystic change and proliferation of the sesamoid bones induced by repetitive impingement on sesamoid bones.
The impingement will increase pressure in the capsule of adjacent synovial joints,
which ultimately results in inflammatory reaction that will lead to tenosynovitis of the flexor tendon,
thickening and fibrosis of the joint capsule.
The sesamoid bones syndrome can be well demonstrated by MRI,
in which we can see bone marrow edema,
soft tissue distention and tendon laceration,
degenerative cystic change signals at the connection area between sesamoid bones and cartilages,
as well as myotenositis of the long flexor muscle of the thumb and effusion within its tendon sheath.
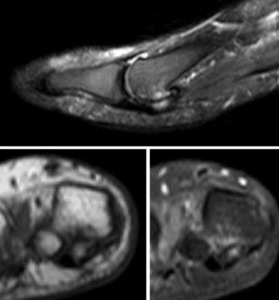
Fig. 7: MRI Sagittal (T2 fat sat) and coronal (T1 and T2 fat sat); Sesamoiditis
References: Department of Radiology, Hospital de São João, Porto, Portugal
Infections
Osteomyelitis affecting the sesamoids is most frequently secondary to direct extension from a soft tissue infection or from a septic joint.
Degenerative disease
The hallucal sesamoids have a true articular joint with the metatarsal head so they are susceptible to osteoarthritis.
Accessory ossicles
Accessory bones result from a non-coalition of several ossification centers or development of extra and independent ossification centers.
The most common accessory bones described in the foot are the os trigonum,
os peroneum and os naviculare.
Os trigonum
Normal anatomy and appearance
Os trigonum is located at the posterolateral aspect of the talus (resulting from a secondary ossification center that appears between the ages of 8 and 13) and can be seen on lateral radiographs of the foot.
Usually it fuses with the talus forming “Stieda process” but when it remains unfused,
it forms a synchondrosis with lateral tubercle of the talus.
Its prevalence is variable ranging from 7 to 25 %.

Fig. 8: Lateral radiography of the foot showing an os trigonum
References: department of Radiology, Hospital de São João, Porto, Portugal
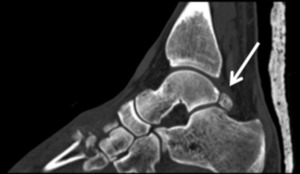
Fig. 9: CT, Sagittal plane demonstrating the normal appearance of os trigonum
References: Department of Radiology, Hospital de São João, Porto, Portugal

Fig. 10: MRI, Sagittal T1; Os trigonum normal appearance
References: Department of Radiology, Hospital de São João, Porto, Portugal
Pathologic conditions
The symptomatic os trigonum may result from an acute or chronic injury and patient always refers a pain with mild swelling of the posterior ankle that is accentuated by resisted plantar flexion or dosiflexion of the great toe.
An acute injury may be caused by trauma and can result in a os trigonum fracture,
although this is a extremely rare condition.
On the other hand,
the chronic injury causing a posterior ankle impingement syndrome is more common and frequently results from excessive plantar flexion of the foot.
So it is easy to comprehend that activities such as ballet can result in this syndrome.
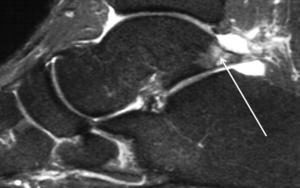
Fig. 11: MRI, T2 fat sat; Os trigonum syndrome
References: Department of Radiology, Hospital de São João, Porto, Portugal
Degenerative changes at the “os trigonum-talus articulation” can also occur resulting in synchondrosis,
local synovitis,
flexor hallucis longus tenosynovitis (as the tendon for the flexor hallucis longus sits medial to the os trigonum in the sulcus between the medial tubercle and the larger lateral tubercle) or intra-articular loose bodies.
Os Peroneum
Normal anatomy and appearance
The os peroneum is located at the cuboid tunnel adjacente to the calcaneocuboid joint and is embedded within the peroneus longus tendon.
It can be best seen in oblique radiographs of the foot and in 30% of the cases it is bipartite.

Fig. 12: Oblique x-ray showing an os peroneum
References: department of Radiology, Hospital de São João, Porto, Portugal
Pathologic conditions
The os peroneum can be involved in painful syndromes as it locates within the peroneus longus tendon.
A tear in this tendon results in lateral pain and tenderness along its course with displacement of the ossicle. Occasionally,
os peroneum can subject to fracture or diastasis of a bipartite os peroneum.
These fractures are particularly difficult to differentiate from bipartite sesamoids and a radiograph made with traction of the peroneus longus tendon can be helpful as it demonstrate diastasis and proximal migration of the fragment.
Accessory navicular
Normal anatomy and appearance
The accessory navicular (or tibiale externum) bone is located at the posteromedial aspect of the foot adjacent to the posteromedial tuberosity of the navicular bone and is one of the most prevalent accessory bones (4-21%).
It is best seen on anterioposterior radiographs of the foot.

Fig. 13: Ankle x-ray showing an accessory navicular bone
References: Department of Radiology, Hospital de São João, Porto, Portugal
Accessory navicular bone can be divided in three types:
- Type I – Is considered to be a sesamoid bone located at the distal posterior tibial tendon
- Type II – The most common one,
locates adjacent to the navicular bone and results from an aufused accessory ossification centre and have a synchondrosis to the navicular tuberosity
- Type III – Is the result of a fused type II accessory navicular bone that results in a prominent tuberosity
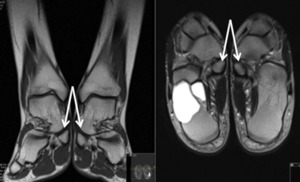
Fig. 14: MRI, Coronal (T1) and axial (T2); Accessory navicular bone (incidental bone cyst on the right talus)
References: department of Radiology, Hospital de São João, Porto, Portugal
Pathologic conditions
Painful accessory navicular is most commonly seen with the type II variant.
It is thought that biomechanical irritation can be the source of the pain with shoe irritation been directly implicated.
This irritation can lead to disruption of the synchondrosis,
posterior tibial tenosynovitis of tibialis posterior or even osteonecrosis.
The tibialis posterior tendon often inserts with a broad attachment into this ossicle.
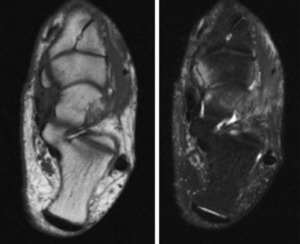
Fig. 15: MRI, Axial T1 and T2 fat sat; symptomatic accessory navicular bone
References: Department of Radiology, Hospital de São João, Porto, Portugal
On MRI we can see an abnormal signal within the ossicle,
in the synchondrosis and navicular tubercle,
within the adjacent soft tissues and in the posterior tibial tendon.
Os intermetatarseum
Normal anatomy and appearance
The os intermetatarseum is located at the intermetatarsal space of the first and second metatarsals and is best seen on an anteroposterior radiograph of the foot.
A very important differential diagnosis has to be made between a normal os intermetatarseum and a Lisfranc injury with fracture of the second metatarsal as the location of these two entities are similar,
but treatment and prognoses are different.
Pathologic conditions
A painful syndrome of the os intermetataeseum is a rare condition and can result from the compression of the superficial or deep peroneal nerve by this ossicle.
The patient complains of dorsal foot pain and numbness at the dorsum of the foot that is exacerbated by standing or jumping,
and tenderness to palpation at the first intermetatarsal interspace.
Os vesalianum
Normal anatomy and appearance
The os vesalium is located at the base of the fifth metatarsal and is embedded in the peroneus brevis tendon and may articulate with cuboid.
It is rare and best seen in oblique radiographs of the foot.
As in the anterior ossicle described is important to differentiate between a normal os vesalium and a fracture of the base of the fifth metatarsal.
Pathologic conditions
A painful syndrome can be seen when a tear of the peroneus brevis tendon occurs,
similarly to that seen in os peroneum with peroneus longus tendon.
Os supranaviculare
Normal anatomy and appearance
The os supranaviculare is rare in prevalence and is located at the dorsal margin of the talonavicular joint space and it can be best seen in lateral foot/ankle radiographs and should not be confused with avultion fracture.
Os supratalare
Normal anatomy and appearance
The os supratalare is located at the dorsal aspect of the talar neck and it can be best seen in lateral foot/ankle radiographs.
This ossicle may be mistaken for flake fractures of the dorsum of the talus resulting from avulsion injuries but its rounded shape is the key for the differential diagnosis.
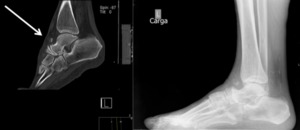
Fig. 16: Sagital TC scan and lateral radiography of the foot showing an os supratalare
References: Department of Radiology, Hospital de São João, Porto, Portugal
Os talotibiale
Normal anatomy and appearance
The os talotibiale is located at the dorsal aspect of the talus adjacent to the talotibiale anterior part of the joint.
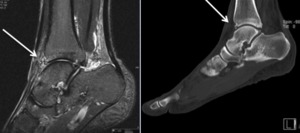
Fig. 17: MRI (Sagittal T2 fat sat) and CT (Sagittal); Os talotibiale
References: department of Radiology, Hospital de São João, Porto, Portugal
Pathologic conditions
These three ossicles are rarely associated with painful syndromes and the most difficult part of their evaluation is their recognition itself.
We have to be aware of their presence to differentiate them from avulsion fractures but the clues are the lack of a donor site,
absent soft tissue swelling and their well corticated margins helping in this differential diagnosis.
Os subfibulare
Normal anatomy and appearance
The os subfibulare is located at the tip of the lateral malleolus (0,2-2%).
Pathologic conditions
The principal consideration of this ossicle is to distinguish it from an acute avulsion fracture of the lateral malleolus.
The os subfibulare is a rounded shaped ossicle with well corticated margins different from the fragment of a fracture that has a sharp fracture margin without sclerosis.
Os subtibiale
Normal anatomy and appearance
The os subtibiale is also rare (0,2-1%) and is located at the tip of the medial malleolus.

Fig. 18: Coronal CT scan showing an os subtibiale
References: Department of Radiology, Hospital de São João, Porto, Portugal

Fig. 19: MRI, Coronal, PD fat sat; os subtibiale
References: department of Radiology, Hospital de São João, Porto, Portugal
Pathologic conditions
Following an acute injury to the ankle the os subtibiale may be mistaken for an isolated medial malleolar avulsion fracture with MRI being once again the method of choice for this distinction.
Os calcaneus secundarium
Normal anatomy and appearance
The os calcaneus secundarium is located at the anterior facet of the calcaneus positioned at the border of the calcaneus,
the cuboid,
the talar head and the tarsal navicular bone.
It is best visualized on oblique foot radiographs or CT scans because of the overlying structures.

Fig. 20: Sagittal CT scan showing an os calcaneus secundarium
References: Department of Radiology, Hospital de São João, Porto, Portugal
Pathologic conditions
The os calcaneus secundarium itself is rarely involved in painful syndromes however an important differential diagnosis have to be made between a normal os calcaneus secundarium and a fracture of the anterosuperior calcaneal process because they look similar on radiographs.
MRI will be the method of choice for this differentiation because it can demonstrate the bone marrow edema of the anterosuperior calcaneal process when a fracture has occurred.
Pathological conditions in sesamoids and accessory ossicles
As a summary,
both sesamoid bones and accessory ossicles can be affected by trauma,
infection,
degenerative disease and osteonecrosis.
Due to their locations in the foot some are more prone than others for different conditions.
- Trauma and fracture - Hallucal sesamoids and the os trigonum;
- Infection - Hallucal sesamoids (direct extension);
- Degenerative disease – Accessory navicular,
os trigonum (accessory ossicles with synchondroses) and os peroneum (embedded within high-use tendons).



 References: Department of Radiology, Hospital de São João, Porto, Portugal")


 and coronal (T1 and T2 fat sat); Sesamoiditis References: Department of Radiology, Hospital de São João, Porto, Portugal")






 and axial (T2); Accessory navicular bone (incidental bone cyst on the right talus) References: department of Radiology, Hospital de São João, Porto, Portugal")


 and CT (Sagittal); Os talotibiale References: department of Radiology, Hospital de São João, Porto, Portugal")


