GENERAL INFORMATION
Traumatic cervical spine injuries belong to the daily routine of emergency radiologist and orthopedic spine surgeon.
With approximate amount of $ 5.6 billion spent yearly for treatment (i.e.
tetraplegia), cervical spine injuries belong to the most costly traumas.
Most common injuries occur in the subaxial cervical spine,
which range from the C3 to C7.
Potential severe complications include dorsal fracture dislocation and spinal cord injury,
which may result in tetraplegia,
neurologic failure and respiratory complications.
For that reason,
meticulous radiological and clinical assessment and consistent reporting systems are needed.
Standardisation of clinical approach and radiological imaging have been proposed (Fig.
2),
however there is still ambiguity concerning classification systems of cervical spine traumas.
Comprehensive nomenclature and structured reporting forms are essential in the acute setting where each moment may be crucial to the patient life and health.
General and musculoskeletal radiologist should be able to provide a consistent report on cervical spine injury that orthopedic spine surgeon would understand even without looking at the images.
To achieve it,
a common classification system for cervical spine traumas should be used both by the radiologist,
and the orthopedic spine surgeon.
THREE COLUMN MODEL OF DENIS
This well-known model was primarily proposed for evaluation of thoracolumbar spinal fractures,
but it can be also used for classification of cervical spine injuries.
According to the Denis classification,
vertebral column can be divided into three columns (Fig.
3 and Fig.
4):
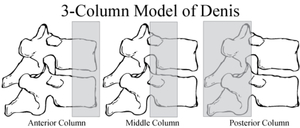
Fig. 3: 3-column model of Denis for vertebral fractures.
References: http://neurosurgerysurvivalguide.com/roundy/
1.
Anterior:
- Anterior 2/3 of the vertebral body and intervertebral space
- Anterior longitudinal ligament
2.
Middle:
- Posterior 1/3 of the vertebral body and intervertebral space
- Posterior longitudinal ligament
3.
Posterior:
- Structures located posteriorly to the posterior longitudinal ligament (facet joints,
spinous processes,
pedicles,
interspinous,
supraspinous and flava ligaments)
Fracture can be classified as unstable when at least 2 of 3 columns are affected.
CLASSIFICATION SYSTEMS
We present three classification systems for cervical spine trauma:
1.
Allen and Fergusson classification
2. Subaxial Cervical Spine Injury Classification System (SLIC)
3.
AOSpine classification (AO- Arbeitsgemeinschaft für Osteosynthesefragen)
Allen and Fergusson (Fig.
5 and Fig.
6)
The classification system was described by Allen and Ferguson in 1982 and has its roots in the era of X-rays.
It is based on suspected mechanism of injury and include:
- Compressive flexion
- Vertical compression
- Distractive flexion
- Compressive extension
- Distractive extension
- Lateral flexion
Subaxial Cervical Spine Injury Classification System (SLIC)
This classification system from 2007 is another commonly used scheme.
It delivers information on:
- Fracture morphology (compression,
burst,
distraction,
translational patterns)
- Quality of disco-ligamentous complex (ligamentous structures,
intervertebral disc,
facet joint capsule)
- Neurological status of the patient
For each of the three categories a different score is given and the sum of the score for all categories is used for therapy management.
Score of 5 or above requires surgical intervention (Fig.
7).
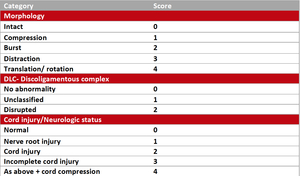
Fig. 7: SLIC
Score of 5 or above indicates a need for surgical treatment
AOSpine classification (Fig.
8)
The AOSpine classification describes injury morphology as follows:
- Type A: Compression
- Type B: Distraction
- Type C: Translation
- Type F: Facet injuries
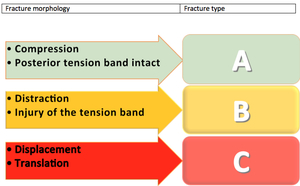
Fig. 8
This classification also mentions neurological status and specific modifiers in the overall evaluation.
Specific modifiers include incomplete disruption of the posterior ligamentous complex,
disc herniation,
vertebral artery injury and the presence of comorbid spine conditions (i.e.
ankylosing spondylitis).
It was established by an expert group of international spine surgeons and is constantly evaluated in ongoing studies.
The last modification was published in 2015.
CHECKLIST FOR A REPORT OF CERVICAL SPINE
To enable a comprehensive and detailed report of the cervical spine injuries different checklists can be used.
We propose a checklist (Fig.
9) with following parameters:
- Alignment (3 columns)
- Fractures (vertebral body,
facet joints,
spinous process)
- Stability of the fracture
- Type of the fracture (i.e.
in the AO classification)
- Spinal cord and canal stenosis
- Ligaments
- Intervertebral space/disc
- Degenerative changes
- Vascular structures (i.e.
vertebral artery)
- Soft tissues
- Others (i.e.
skull base,
pneumothorax)

Fig. 9: Checklist for an exemplary report of cervical spine injury (radiographs, CT, MRI)

 and NEXUS criteria (National Emergency X-Radiography Utilization Study). Both studies describe a decision management in patients with trauma and specify the rules for performing radiographs of the cervical spine.")
.")

References: Urrutia J, Zamora T, Campos M et al (2016) A comparative agreement evaluation of two subaxial cervical spine injury classification systems: the AOSpine and the Allen and Ferguson schemes. Eur Spine J 25:2185-2192")
 References: Urrutia J, Zamora T, Campos M et al (2016) A comparative agreement evaluation of two subaxial cervical spine injury classification systems: the AOSpine and the Allen and Ferguson schemes. Eur Spine J 25:2185-2192")
")