Ligament injuries of the ankle are among the most common injuries in the active population. Between them,
deltoid ligament injuries occur more often than generally believed,
with complete tears being occasionally seen in association with lateral malleolar fractures or bimalleolar fractures,
whose incidence has increased in the last decades [1].
The deltoid ligament is responsible for medial stabilization of the ankle,
limiting the anterior,
posterior and lateral translation of the talus in the talocrural joint,
with its deep bundle being the main blocker of the external rotation and the most important contributor to the stability of the ankle.
[2,3,4]
Any malleolar fracture associated with ligament rupture should so be considered unstable and consensually surgically treated in order to restore the anatomy and stability of the ankle.
[5,6,7,8]
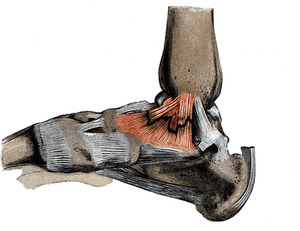
Fig. 1: Illustration of the ligaments of the medial aspect of the foot with schematic deltoid ligament rupture.
References: Adapted from Henry Gray (1918) Anatomy of the Human Body
In the acute setting of trauma,
the primary evaluation is made by plain radiography and ultrasound,
with medial clear space widening on a mortise radiograph suggesting ligamental injury and instability of the ankle fracture.
Stress radiographs,
as the Manual External Rotation Stress View (MERS) or the Gravity Stress View (GS),
are considered helpful to gain indirect evidence of lesions of the deltoid ligament.
Even though the manual stress test has been classically used,
it is difficult to standardize and is not always tolerated by the user,
and so its practicality has been questioned.
Michelson et al. [5] and Gill et al. [7] recommend the gravitational stress test instead,
considering it as reliable as the manual external rotation stress test,
but having the advantage of less exposure to ionizing radiation.
Notwithstanding,
some authors have also warned that gravitational stress radiography overestimates the results [19].
Consequently,
there's still no consensus as to the best instrument to be used as a method of assessing the integrity and competence of the deltoid ligament.
[13,14,15,16]
When such tests are used to distinguish between individuals with normal (no lesion) or abnormal (with lesion) results,
it is important to understand how the characteristics are distributed across populations,
and also necessary to determine the cut-off point above which the test is considered positive and below which it's considered negative.
[9]
Previous studies by McConnel,
Gill,
Schock,
and DeAngelis determined that a medial clear space ≥4 mm,
or a superior space ≥1 mm,
on radiography at 10° internal rotation,
is indicative of rupture of the deltoid ligament bundles.
[6,7,8,10] Park in 2006, in her study on six corpses, suggests that a medial clear space ≥5 mm has a higher predictive value in determining the degree of instability.
[11] And,
since clinical decisions are often based on differences between millimeters,
it is also crucial to understand the agreement in the measurement,
with works on corpses by Metitiri and Ghorbanhoseini warning for a high degree of error and inaccuracy in measurements.
[12]
Thus the main PURPOSE of this prospective study was:
- to determine the validity and reliability of the Manual External Rotation Stress test when compared to the Gravity Stress test,
concerning deltoid ligament injury in isolated lateral ankle fractures.
and secondarily:
- to evaluate whether the medial clear space ≥4 or ≥5 mm has different predictive value for deltoid ligament injury;
- to assess the reliability of the measurements.
