ESTI 2019 / P-0024
Thoracic imaging findings in patients with primary humoral immunodeficiency.
Congress:
ESTI 2019
Poster Number:
P-0024
Type:
Educational Poster
Keywords:
Inflammation, Infection, Genetic defects, Education, Complications, Plain radiographic studies, CT, Conventional radiography, Thorax, Respiratory system
Authors:
P. Patel, I. Karafotias, S. D. Tran, N. Mulholland, G. Yusuf, K. Stefanidis; London/UK
DOI:
10.26044/esti2019/P-0024

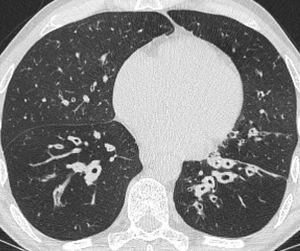
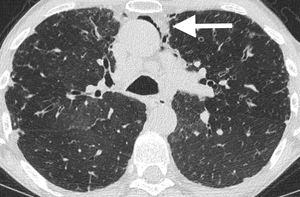
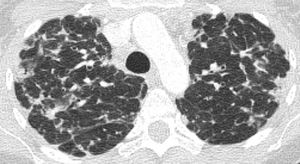
Fig. 1:
This CT demonstrates focal ground glass opacities. This patient had a diagnosis...

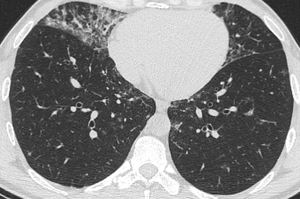
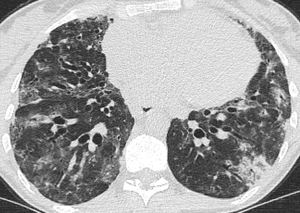
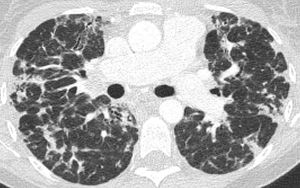
Fig. 2:
In the same patient with XLA there is lower lobe bronchiectasis and bronchial...

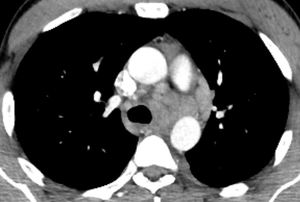
Fig. 3:
Axial CT image showing segmental right upper lobe consolidation in a patient...

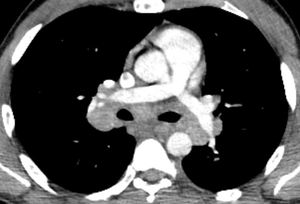
Fig. 4:
In the same patient with CVID there is lower lobe bronchiectasis.

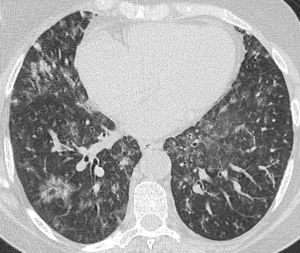
Fig. 5:
Axial CT image in a patient with CVID showing multiple micronodules with patchy...

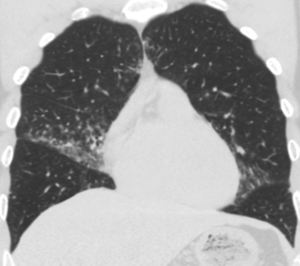
Fig. 6:
Coronal reconstruction in the same patient with CVID depicting the mid zone...

Fig. 7:
Upper zone image from a CT chest of a patient with CVID and recurrent...

Fig. 8:
Mid zone image from a CT chest of the same patient with CVID demonstrating the...

Fig. 9:
Lower zone image from a CT chest of the same patient with CVID and recurrent...

Fig. 10:
Cylindrical lingual, lower and middle lobe predominant bronchiectasis with...

Fig. 11:
Complication of recurrent infections with pneumomediastinum in the same ...

Fig. 12:
Cylindrial bibasal bronchiectasis and bronchial wall thickening in a patient...

Fig. 13:
Axial CT image of a patient with a granulomatous variant of CVID demonstrating...

Fig. 14:
Axial CT image on mediastinal windows, which demonstrates mediastinal and hilar...

Fig. 15:
Further axial CT image on mediastinal windows in the same patient demonstrating...

Fig. 16:
Coronal reconstruction on mediastinal windows in the same patient showing the...

Fig. 17:
Upper zone axial CT chest image in a patient with CVID, which shows extensive...

Fig. 18:
Mid zone axial CT chest image in the same patient with CVID.

Fig. 19:
Lower zone axial CT chest image in the same patient with CVID showing the...

Fig. 20:
This is an example of Good's syndrome in a patient with hypogammaglobulinaemia....

Table 1:
Correlation of the subtypes of the various primary immunodeficiencies with the...

Table 2:
Correlation of the subtypes of the various primary immunodeficiencies with the...