ESTI 2019 / P-0071
Lungs of stone – a review of pulmonary calcification and other causes of high attenuation lesions in the lungs
Congress:
ESTI 2019
Poster Number:
P-0071
Type:
Educational Poster
Keywords:
Calcifications / Calculi, Diagnostic procedure, CT-High Resolution, CT, Lung
Authors:
L. Chen1, V. Halai2, A. Leandru3, A. Wallis1; 1Portsmouth/UK, 2Waterlooville/UK, 3Portsmouth, UK/UK
DOI:
10.26044/esti2019/P-0071

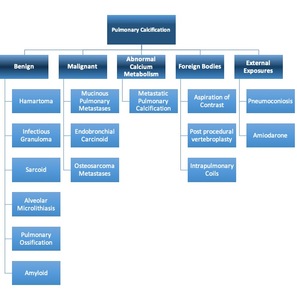
Table 1:
Causes of pulmonary calcification

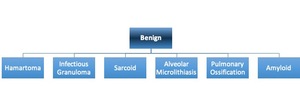
Table 2:
Benign causes of pulmonary calcification

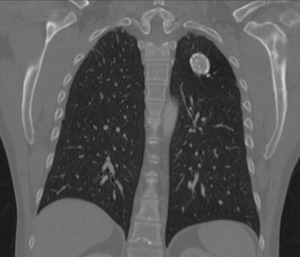
Fig. 1:
Left upper lobe calcified granuloma
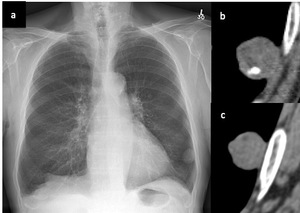
 and on CT imaging to contain calcification (b) and fat (c) in keeping with a hamartoma.")
Fig. 2:
Left lower lobe subpleural shown here on chest x-ray (a) and on CT imaging to...

Fig. 3:
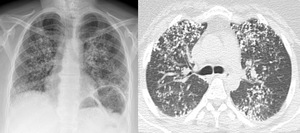
Lung and mediastinal windowed images of a patient with bilateral perilymphatic...

Fig. 4:
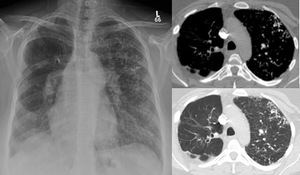
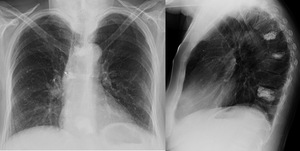
Chest x-ray demonstrating upper lobe predominant nodularity and CT chest slice...

Fig. 5:
Chest radiograph shows right lung allograft and the left native lung has...

Fig. 6:
Calcified and non calcified pulmonary nodules on CT chest in keeping with...

Table 3:
Malignant causes of pulmonary calcification.

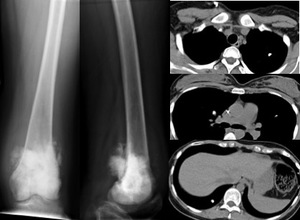
Fig. 7:
AP and lateral radiographs of the left femur demonstrating an ill defined...

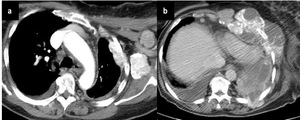
Fig. 8:
Two CT chest slices. Figure 8a shows avidly enhancing and partially calcified...
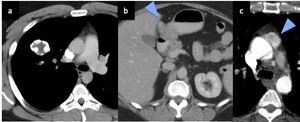
 shows a right lung pulmonary chondroma with peripheral calcification, (b) shows an arrow indicating towards a pyloric gastrointestinal stromal tumour and (c) shows an arrow pointing towards an extra adrenal mediastinal paraganglioma.")
Fig. 9:
Carney’s triad: (a) shows a right lung pulmonary chondroma with peripheral...

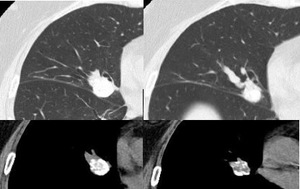
Fig. 10:
Lung and soft tissue windows of two slices through a peripherally calcified...

Table 4:
Abnormal calcium metabolism

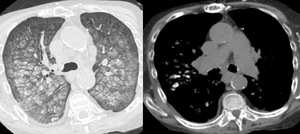
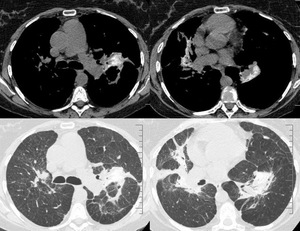
Fig. 11:
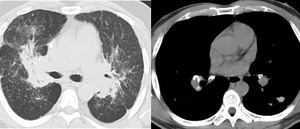
Centrilobular nodules and ground glass of calcific attenuation in keeping with...

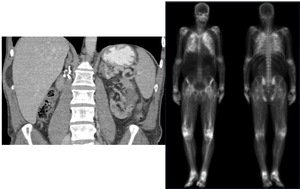
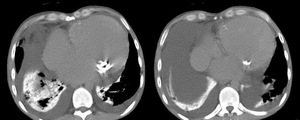
Fig. 12:
Coronal CT upper abdomen showing surgical clips in the right nephrectomy bed...

Table 5:
Foreign bodies causing pulmonary calcification or high density
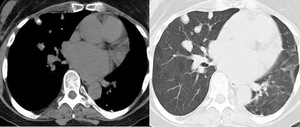
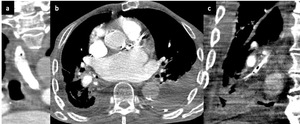
. Oral contrast has been aspirated and fills the the right lower lobe bronchi (b) and coronal reformat of the right lower lobe bronchi shows contrast with locules of gas, with distal atelectasis and consolidation (c).")
Fig. 13:
CT Chest demonstrating a contrast filled oesophagus (a). Oral contrast has been...

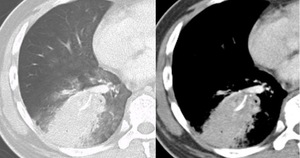
Fig. 14:
Lung and mediastinal window CT images of the right lower lobe a high...
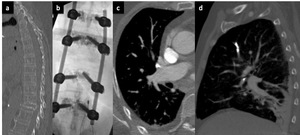
 Sagittal thoracic spine on bone windows shows a lower thoracic vertebral collapse with fluoroscopy of spinal fixation (b) and very dense material within the upper lobe arteries on CT (c) and (d).")
Fig. 15:
(a) Sagittal thoracic spine on bone windows shows a lower thoracic vertebral...

Fig. 16:
Chest x-ray and lateral thoracic spine x-ray showing high density parenchymal...

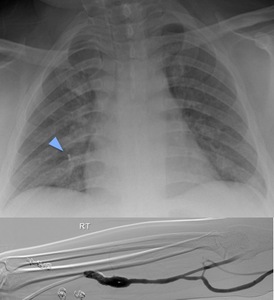
Fig. 17:
Chest x-ray with arrow indicating a metallic coil and peripheral angiogram of...

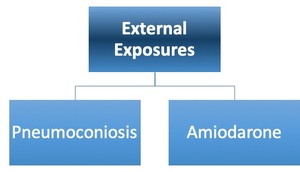
Table 6:
External exposures causing high attenuation within the lungs.

Fig. 18:
Unenhanced CT Chest demonstrating calcified perhilar progressive massive...

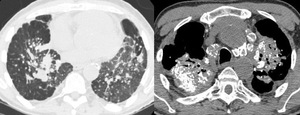
Fig. 19:
Talcosis demonstrated on mediastinal and lung windows with fine high density...

Fig. 20:
CT chest slices demonstrating cardiomegaly, mitral annulus calcification and...