Mosaic attenuation (Inhomogeneous lung opacity) is a term of describing computed tomography (CT) imaging pattern.
It is used to describe when inhomogeneous areas of differing lung attenuation are seen.
Definition suggested by Fleischner society is ‘‘Patchwork of regions of differing attenuation seen on CT of the lungs”.
Originally it was called as “mosaic oligemia and perfusion”.
But mosaic attenuation is more inclusive term,
and mosaic oligemia or mosaic perfusion implies ‘pulmonary vascular pathology’.
Normal lung attenuation on chest CT
Not only air but also blood attributes approximately half of the normal lung attenuation on CT.
When amount of air is increased,
the attenuation of the lung is decreased (air trapping).
Otherwise,
when blood flow is increased,
the attenuation of the lung is also increased.
Furthermore,
other pathologic condition such as water (pulmonary edema),
inflammatory cell (pneumonia),
malignant cell (tumor) can increase lung attenuation
Parenchymal inhomogeniety in lung.
Increased or decreased lung attenuation on chest CT shows parenchymal inhomogeneity of lung attenuation.
Determining which areas (‘increased area’ or ‘decreased area’) of lung attenuation are normal or abnormal is major difficulty,
when you face on the mosaic attention pattern. (Fig.
1).
There are several normal parenchymal inhomogeniety on normal individuals.
Most dependent portion of the lung shows slightly higher attenuation,
and posterior aspect of upper lobes often shows higher attenuation than the superior segment of the lower lobes.
Because of the physiologic perfusion gradient,
central portion shows slightly higher attenuation than the peripheral portion of the lung.
Up to twenty percent of normal patient,
mild mosaic attenuation involving smaller than a segment can be seen.
Abnormal parenchymal inhomogeniety result in 1) abnormally decreased attenuation area,
2) abnormally increased attenuation area,
or 3) mixed abnormally decreased and increased area
Predominant cause of mosaic lung attenuation
Abnormally decreased attenuation area is usually due to small airway disease (air trapping) or pulmonary vascular disease (mosaic perfusion).
Abnormally increased attenuation area is due to lung parenchymal disease (ground-glass opacity or consolidation).
Small airway disease
Definition of small airway is non-cartilaginous airways with internal diameter below 2mm or 8th generation of airways down to terminal & respiratory bronchioles.
It is normally non-visible on CT,
but visible due to underlying disease.
Pathophysiology of the low attenuation area is when there is an obstruction of a small airway, in spite of aeration through collateral airflow (pores of Kohn,
canals of Lambert,
channels of Martin),
ability of adequate gas exchange is reduced in involved lung and result in reflex hypoxic vasoconstriction which means blood is shunted away (Fig. 2).
This mechanism decrease blood perfusion and more lucent appearance with decrease size of vasculature and even decreased number of vasculature (Fig.
3)

Fig. 2: 56-year-old woman with constrictive bronchiolitis obliterans. Expiratory CT scan at the level of subcarina shows low attenuation areas in both lower lobes, lingular segment (star). Anterior bowing of posterior wall of right bronchus intermedius reveals end-expiratory status (arrow).
References: courtesy of Dr. Yoon-young Choi.
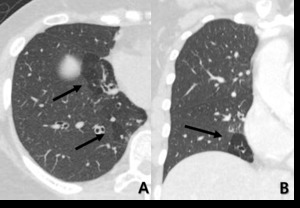
Fig. 3: 50-year-old woman with small airway disease and bronchiectasis. On inspiratory CT scan, transaxial scan shows low attenuated area with decreased vascularity and combined bronchiectatic change (arrow), (B) coronal reconstructed image shows well defined bronchiolectasis within lobular hypoattenuated area wtih decreased vascularity at the same level of (A).
Pulmonary vascular disease.
Mosaic pattern attenuation is due to regional differences in blood perfusion.
Two main diseases are pulmonary artery hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH).
PAH is a disease that primary abnormality in distal pulmonary arterioles and vasoconstriction in peripheral pulmonary arteries.
CTEPH is result from organizing thrombi in elastic pulmonary arteries,
which leads partial or complete vascular occlusion (Fig.4).
Both PAH and CTEPH,
in consequence,
decreases blood flow in the regional area lung and reduced attenuation in the same area.
Multiple hematogenous metastatic tumor emboli lodges and occludes lobular bronchiole or lobular arterioles,
represents lobular low attenuation in the area of lobule due to decreased blood flow to distal regional lung (Fig.5)

Fig. 4: 71-year-old woman with chronic thromboembolic pulmonary arterial hypertension. (A) Right lobar pulmonary contains eccentric wall calcifications resulted from chronic pulmonary arterial thromboembolism (arrow). (B) At the same level of (A), bilateral hypoattenuated area of both superior segment of lower lobe noted as sequence of decreased blood flow in distal region.
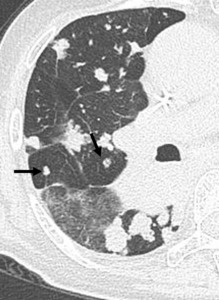
Fig. 5: 69-year-old woman with multiple lung metastasis from rectal cancer.
Multiple hematogenous metastatic tumor emboli lodge and occlude pulmonary arteries (arrow) in the central core and surrounding lobular hypoattenuated region are defined.
Parenchymal disease
Ground glass opacity (GGO) is increased lung attenuation through which underlying airway and vessels remain visible (Fig.6).
There is a lot of etiology to induce GGO.
Pathophysiology are thickening of alveolar wall due to inflammation or fibrosis,
alveolar collapse,
increased capillary blood volume,
presence of fluid,
cells,
amorphous material partially filling alveolar spaces,
and combination of these.
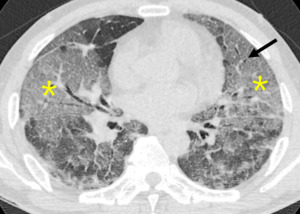
Fig. 6: Increased attenuation composed of ground glass opacity or consolidation, represents air-space filled lesions and interstitial thickenings or air-space wall thickenings, sometime shows air-bronchogram

. Black areas note decreased (hypoattenuated) lung(B); white areas note increased (hyperattenuated) lung(C).")
. Anterior bowing of posterior wall of right bronchus intermedius reveals end-expiratory status (arrow). References: courtesy of Dr. Yoon-young Choi.")
, (B) coronal reconstructed image shows well defined bronchiolectasis within lobular hypoattenuated area wtih decreased vascularity at the same level of (A).")
 Right lobar pulmonary contains eccentric wall calcifications resulted from chronic pulmonary arterial thromboembolism (arrow). (B) At the same level of (A), bilateral hypoattenuated area of both superior segment of lower lobe noted as sequence of decreased blood flow in distal region.")
 in the central core and surrounding lobular hypoattenuated region are defined.")
