ESTI 2019 / P-0112
Diagnosing Idiopathic Pulmonary Fibrosis according to updated 2018 diagnostic criteria guidelines: a case-based pictorial review
Congress:
ESTI 2019
Poster Number:
P-0112
Type:
Educational Poster
Keywords:
Inflammation, Biopsy, CT, Thorax, Lung
Authors:
M. Benegas Urteaga1, M. Sanchez1, I. Vollmer2, F. Hernandez 2, C. Lucena 2, J. Ramirez1, J. Sellares1; 1Barcelona/ES, 2Barcelona /ES
DOI:
10.26044/esti2019/P-0112

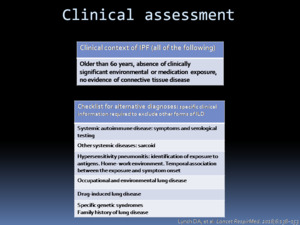
Fig. 1:
Clinical assessment according to Fleischner guideline. It is essential to...

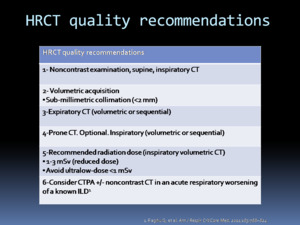
Fig. 2:
HRCT scanning recommendations for the accurate diagnosis of IPF.

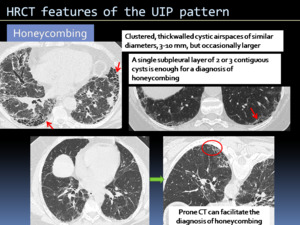
Fig. 3:
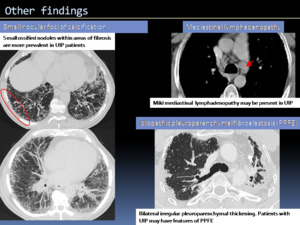
HRCT features of the UIP pattern.

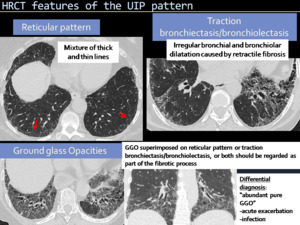
Fig. 4:
HRCT features of the UIP pattern.

Fig. 5:
HRCT features of the UIP pattern.

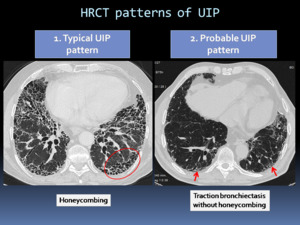
Fig. 6:
HRCT patterns of UIP: Typical UIP pattern and Probable UIP pattern.

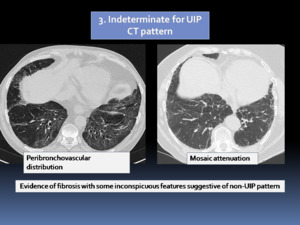
Fig. 7:
HRCT patterns of UIP: Indeterminate for UIP CT pattern.

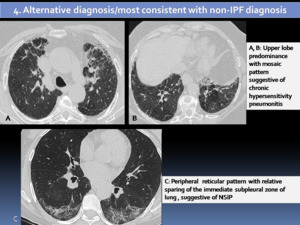
Fig. 8:
HRCT patterns of UIP: Alternative diagnosis/most consistent with non-IPF...
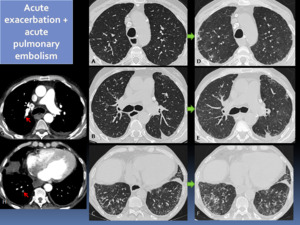
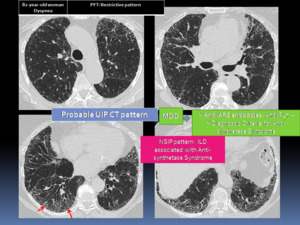
 who presented with acute respiratory worsening. HRCT and chest CT angiography were performed showing new bilateral GGOs (D-F) and segmentary acute pulmonary embolism (G-H).")
Fig. 9:
75 year-old-man with a probable UIP pattern (A-C) who presented with acute...

Fig. 10:
Comparison of HRCT UIP patterns with the characteristic CT features according...

Fig. 11:
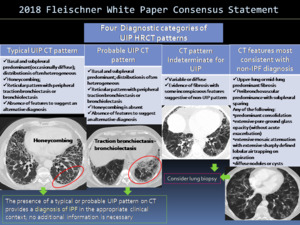
Four diagnostic categories of UIP based on CT patterns according to 2018...

Fig. 12:
Four diagnostic categories of UIP based on CT patterns according to 2018...

Fig. 13:
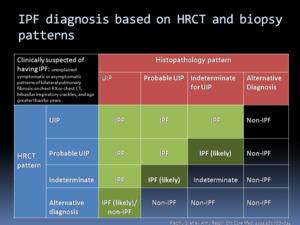
IPF diagnosis based on HRCT and histopathology patterns.

Fig. 14:
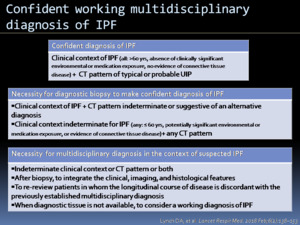
Confident working multidisciplinary diagnosis of IPF according to Fleischner...

Fig. 15:
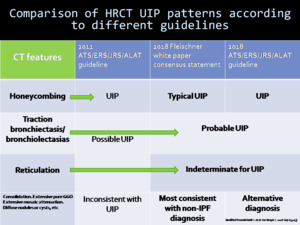
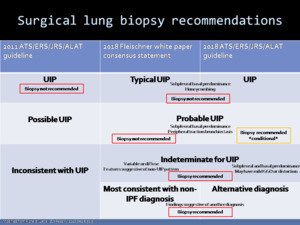
Comparison of HRCT UIP patterns according to different guidelines and the...

Fig. 16:
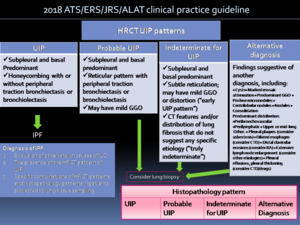
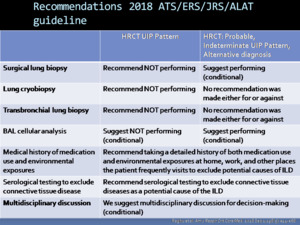
Recommendations for the diagnosis of IPF detailed in the 2018 ATS/ERS/JRS/ALAT...

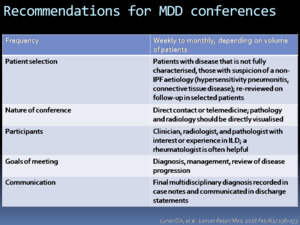
Fig. 17:
MDD: multidisciplinary discussion. Recommendations for MDD conferences...

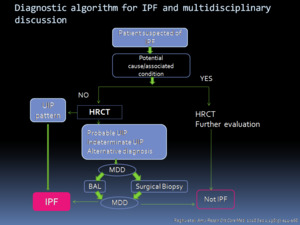
Fig. 18:
Diagnostic algorithm for IPF proposed in the 2018 ATS/ERS/JRS/ALAT guideline.

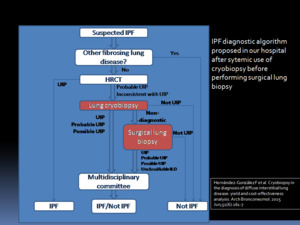
Fig. 19:
IPF diagnostic algorithm proposed in our hospital after sytemic use of...
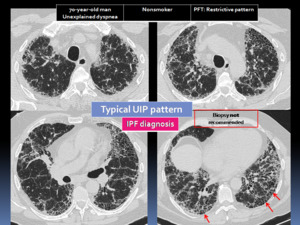
 with basal and subpleural reticular pattern and peripheral traction bronchiectasis. Theses features correspond to a typical UIP pattern, representing an IPF diagnosis. Biopsy is not recommended.")
Fig. 20:
70-year-old man with unexplained dyspnea. Axial HRCT images show the presence...
 with a reticular pattern. Honeycombing is not present. A surgical lung biopsy (SLB) was performed and UIP was proven at histology.")
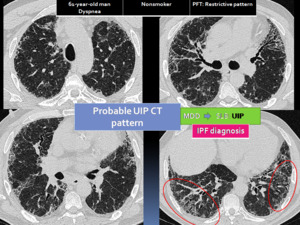
Fig. 21:
61-year-old man with dyspnea. Probable UIP pattern: Axial HRCT images show...
 . A surgical lung biopsy (SLB) showed probable UIP (A: subpleural and paraseptal distribution of fibrosis with architectural distortion; B: higher power evaluation showing patchy fibrosis without honeycomb change. Based on HRCT and biopsy pattern proposed in the 2018 ATS/ERS/JRS/ALAT guideline, the patient was diagnosis with IPF (likely), considered in this case an “Early usual interstitial pneumonia”.")
Fig. 22:
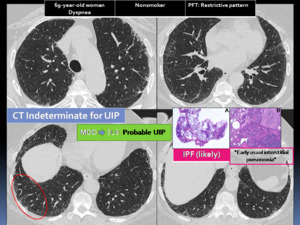
69-year-old woman with dyspnea. Indeterminate for UIP CT pattern (reticular...
 and mosaic attenuaction pattern. Relevant clinical information suggestive of chronic hypersensitivity pneumonitis (CHP) was highlighted in the MDD: Suspicious domestic exposure; Elevated IgG for Aspergillus, Cladosporium, Penicillium; Bronchioloalveolar lavage: M 62% N 35% L 3%. A cryobiopsy was non-diagnostic. A surgical lung biopsy (SLB) was performed demonstrating A: interstitial fibrosis centered and extending around the bronchioles without non-necrotising granulomas, suggesting a CHP.")
Fig. 23:
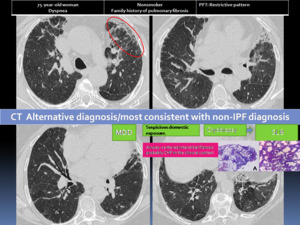
75-year-old woman with dyspnea. HRCT with features of an alternative diagnosis:...
 and diagnostic criteria for Anti-synthetase Syndrome. The HRCT pattern was considered as a Nonspecific interstitial pneumonia (NSIP) related to the autoimmune disease.")
Fig. 24:
A 82-year-old woman with dyspnea and a probable CT pattern was presented in a...