All the children investigated in our department in the last 5 years are explored by ultrasound first, ultrasound being also the follow-up technique. We use ultrasound informations as a base for the following investigations. In the past, we used conventional urography, but the X-ray exposure was significant (especially in old equipment) and the results were frequently inconclusive, sometimes even ambiguous, additional CT exams being necessary for a complete imaging diagnosis, so we have decided to replace this method with CT urography.
Our continuous concern was to obtain maximum imaging information with minimum X-ray exposure. That’s why we now use CT urography (CTU) as an additional tool for an accurate imaging diagnosis, especially in potentially surgical cases, but we adapt our technique in order to reduce radiation dose. Most of the children have been investigated on a 16 sliced CT equipment but some of them have been explored on a 4 slices CT machine. We performed split-bolus CT scan in 8 children but we included in our study only 7, 3 boys and 4 girls, with ages between 8 and 17 years (one child was cachectic for his age so we couldn’t find a similar child to compare).
Split Bolus CT urography (SBCTU) protocol
The child must be placed in the centre of the gantry because we use a single scanogram (only frontal scanogram).
We first perform a NECT phase representing the equivalent to KUB (Kidney, ureter and bladder X-ray), in order to recognize lithiasis and vascular calcification. Then we perform a single-phase CECT representing the equivalent of conventional urography.
Technical parameters have been adjusted according to age and weight, the pediatric protocols in use being recognized by colours, each colour representing a specific body weight interval. The physical parameters used for split-bolus CT are tube voltage and tube current (mA). For dose reduction, we can use a tube voltage between 80-100 kV especially in children with a weight under 40-45 kg. All pediatric X-ray exams need automatic exposure control (AEC) if available in order to adjust radiation dose to child morphotype.
For CECT examination, we inject 1.5-2 ml/kgc of iodinated contrast with a concentration of 300 mg/iodine ml (between 300-400 mg iodine/ml), but we split the contrast into two fractions: we first injected half amount of contrast, we waited 420 seconds (or more, depending of the obstruction degree seen on ultrasound), then we injected the last half amount by an automatic injector (see the table below). Between the first and second part of the injection, we can inject a diuretic drug (Furosemide), unless we suspect an obstructive urinary condition. We do not use it currently in children because many pacients have suspected obstructive-malformative conditions but it is useful to include it in the standard protocol because it can reduce artifacts caused by high iodine concentration. The CECT was performed 80-90 seconds after injection start without using bolus tracking. We obtained a twice opacification (parenchymal and urinary pathways opacification) with a single injection. In complex pediatric cases, we used a different technique consisting in two-phase CECT (one corticomedullary and one excretory phase) but in big children with US suspected vascular or tumoral pathology we used the adult technique (three-phase kidney).
The radiation dose (DLP) is reported in mGy*cm.
|
SBCT
|
Unenhanced CT (NECT)
|
Enhanced CT (CECT)
|
|
Physical parameters (KV, mA)
|
80-100 KV, reduced mA
|
80-100 KV, reduced mA
|
|
Pitch
|
Under 1
|
Under 1
|
|
Collimation
|
Necessary (thin)
|
Necessary (thin)
|
|
Automatic exposure control (AEC)
|
Yes
|
Yes
|
|
Investigation segments
|
Abdominal and pelvic
|
Abdominal and pelvic
|
|
Start position
|
Xiphoid appendix
|
Xiphoid appendix
|
|
End position
|
Pubic symphysis
|
Pubic symphysis
|
|
Contrast medium type
|
Not applied
|
Non-ionic iodinated contrast
|
|
Contrast medium concentration
|
Not applied
|
300-400 iodine/ml (preferable 300 ml iodine/ml)
|
|
Injection rate
|
Not applied
|
1,5-2 ml/sec
|
|
Amount of iodinated contrast
|
Not applied
|
1,5-2 mg/kgc
|
|
Voice command
|
Off
|
Off
|
|
Slice thickness
|
5 mm
|
5 mm
|
|
Thin reconstruction
|
1,25 mm
|
1,25/2,5 mm
|
|
MPR/VRT
|
IF necessary
|
Yes (during interpretation)
|
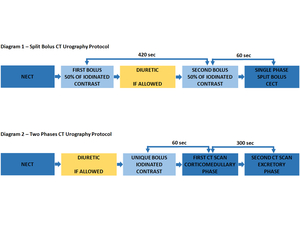
Fig. 1
Results
We compared the radiation dose between group A representing patients investigated through one-phase split-bolus CT urography and group B representing children investigated through two-phases CT urography (Table 1, 3) for similar ages and weight (if available) and we also compared the radiation dose between group A and group C, group C representing pediatric patients investigated through another CT scan protocol for renal or extrarenal pathology (Table 2, 3).
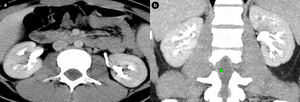
Fig. 2: Girl, 15 yo - Single-phase split bolus CT urography a,b. Axial (a) and coronal (b) plane - normal nephrogram (symmetrical, homogenous enhancement of the renal parenchyma) with normal urogram (symmetrical opacification of urinary collecting system) after double iodinated contrast injection.
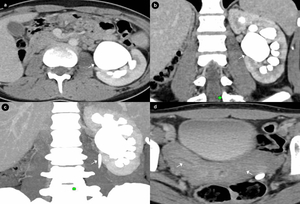
Fig. 3: Girl, 17 yo - Single-phase split-bolus CT urography a. cortico-medullary and excretory phase and b. MPR (coronal plane) showing solitary left kidney (absence of the right kidney) and left pyeloureteral junction obstruction (PUJO) with HN grade II-III (arrows); c. MIP (coronal plane) - showing decalibration at the level of pyeloureteral junction with thin lumbar ureter (arrow); d. bicornuate uterus (arrows), a classic association with renal agenesis.
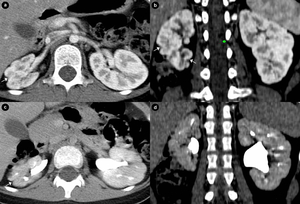
Fig. 4: Girl, 8 yo - Two-phases CT urography a,b. corticomedullary phase - axial (a) and coronal (b) plane; c,d. excretory phase - axial (c) and coronal (d) plane - right hypotrophic kidney with multiple contour irregularities and focal reduction of parenchymal thickness representing small renal scars (arrows) secondary to multiple upper urinary tract infection (cronic pyelonephritis).
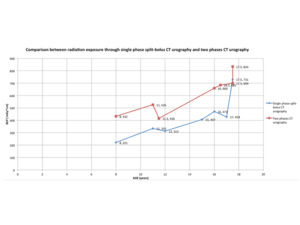
Table 1
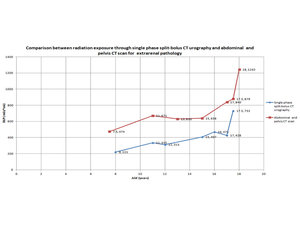
Table 2
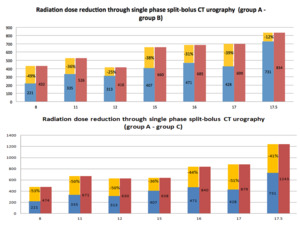
Table 3
Discussions
This protocol consisting in a NECT and a single-phase CECT of conventional urography can successfully replace the old imaging methods. The image quality is satisfactory in most of the cases but sometimes, we have artifacts in the renal parenchyma caused by the iodinated contrast so for the future it is recommended to use iodinated contrast with 300 ml iodine/ml. However, reduction dose is significant in most of the cases and is significantly  higher in the second situation (group C comparing to group A). Sometimes the obstructive pathology can lead to a significantly delayed excretion, so in rare cases we must perform a delayed CT phase for an accurate diagnosis. Even if SBCT is a valuable diagnosis tool, we do not perform control CT scans in children unless we have a very well justified indication.
higher in the second situation (group C comparing to group A). Sometimes the obstructive pathology can lead to a significantly delayed excretion, so in rare cases we must perform a delayed CT phase for an accurate diagnosis. Even if SBCT is a valuable diagnosis tool, we do not perform control CT scans in children unless we have a very well justified indication.
Main indications for SBCTU are:
- complicated lithiasis in the stages prior to ESWL or surgical treatment;
- complicated malformative reno-urinary disease - for example duplicated collecting system associating obstruction-pyeloureteral junction obstruction - (PUJO)/vesico-ureteral junction obstruction (VUJO), megaureter, obstructive ureterocele etc;
- differential diagnosis between multicystic dysplastic kidney, polycystic kidney disease and severe/atypical hydronephrosis;
- ambiguous cystic lesions (except malignant transformation).
Advantages of SBCTU:
- complete diagnosis of malformative - obstructive disease in children;
- reduced radiation exposure;
- small time of investigation comparing to MRI.
Limitations:
- incomplete investigation of vascular pathology (stenosis/thrombosis) or tumoral pathology;
- X-ray exposure (reduced, but still present);
- useless in vesicoureteral reflux (VUR).
Structured result for SBCT urography result must include the following:
Kidneys:
- number, position, dimensions;
- corticomedullary differentiation, symmetrical excretion;
- presence/absence of lithiasis;
- presence/absence of hydronephrosis (obstructive - lithiasis/PUJO);
- presence/absence of malformative/inflammatory/cystic/tumoral pathology.
Ureters:
- unique/multiple (bifid ureters, duplicated collecting system);
- dilated ureters (magaureter) through obstructive lithiasis/ureterocele/VUJO/vesico-ureteral reflux (VUR);
- aberrant insertion of the ureter into prostate, prostatic urethra/seminal vesicle, vagina etc.
Bladder:
- position, size, repletion degree;
- walls (global thickening-UTI)/focal thickening), additional images, lacunar images;
- content (urine, blood clots).
Anatomical variants of renal pedicles
Incidentalomas


 and coronal (b) plane - normal nephrogram (symmetrical, homogenous enhancement of the renal parenchyma) with normal urogram (symmetrical opacification of urinary collecting system) after double iodinated contrast injection.")
 showing solitary left kidney (absence of the right kidney) and left pyeloureteral junction obstruction (PUJO) with HN grade II-III (arrows); c. MIP (coronal plane) - showing decalibration at the level of pyeloureteral junction with thin lumbar ureter (arrow); d. bicornuate uterus (arrows), a classic association with renal agenesis.")
 and coronal (b) plane; c,d. excretory phase - axial (c) and coronal (d) plane - right hypotrophic kidney with multiple contour irregularities and focal reduction of parenchymal thickness representing small renal scars (arrows) secondary to multiple upper urinary tract infection (cronic pyelonephritis).")


