Congress:
EuroSafe Imaging 2020
Keywords:
Performed at one institution, Observational, Retrospective, Embolism / Thrombosis, Audit and standards, CT-Angiography, Conventional radiography, Pulmonary vessels, Lung, Emergency, Action 1 - Guidelines, implementation policies, and Clinical Decision Support (ESR iGuide)
Authors:
M. Al-Mahtot, N. McCarville, A. Tighilt, K. Luckyram, D. Hakim, P. Bamania
DOI:
10.26044/esi2020/ESI-09704
Background/introduction
Pulmonary embolism (PE) has an annual incidence of 78/10,000 in the UK1. CT pulmonary angiogram (CTPA) provides a sensitive and specific means of diagnosing PE, when supported by strong clinical judgement and the modified Wells score for PE (Figure 1) as outlined in the NICE guidance1. The modified Wells score provides a pre-test probability of the likelihood of PE2. NICE and BTS guidelines outline that a chest x-ray is useful prior to CTPA in ruling out alternative diagnoses3. Our local trust guidelines state this as a requirement as well4. It is advised that CTPA scans be performed instead of V/Q scans in patients with abnormal chest x-ray findings as these abnormalities can affect interpretation of a V/Q scan5. D-dimer assay is a valuable diagnostic and a negative test reliably excludes PE in patients with low to intermediate clinical probability of PE3. It is worth noting that in those with high clinical probability of PE d-dimer should not be done and investigation should proceed straight to imaging3. There is concern that CTPA scans are overused as a diagnostic tool. Therefore, we examine whether the Wells score and chest x-rays are utilised as first step investigations to identify suitable patients for a CTPA scan in a District General Hospital (DGH) in Surrey, in order to avoid inappropriate scans.
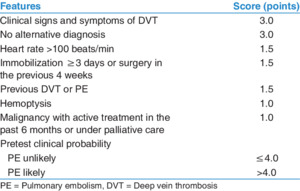
Fig. 1: The modified Wells
score for PE.
References: https://www.researchgate.net/fi gure/Modified-Wellscriteria_tbl1_309719130
