Of the 420 studied cases of HC we found complications in 48 patients (11,42%), several of them presenting concomitant complications. In all of the cases the primary HC was hepatic.
The spectrum of complications comprises:
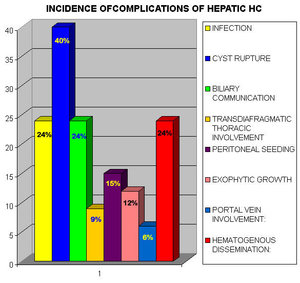
Fig.
1. INTRAHEPATIC COMPLICATIONS
A. Cyst rupture: 40%
Contained: occurs when the endocyst ruptures but the pericyst remains intact. The serpent sign is present: detached undulating membranes (colapsed endocyst) inside the HC without the reduction in the cyst size.
Communicating: implies passage of the cyst contents into the biliary radicles that have been incorporated into the pericyst.
Direct: occurs when both the pericyst and endocyst rupture, allowing free passage of hydatid material into the peritoneal cavity, pleural cavity, hollow viscera, abdominal wall...

Fig.
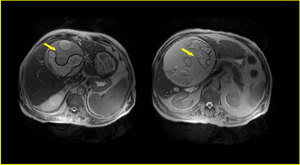
Fig.
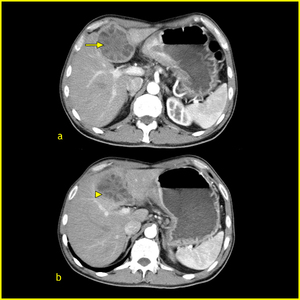
Fig.
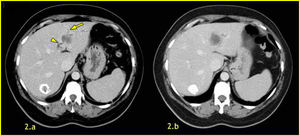
Fig.
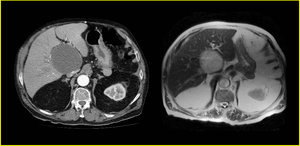
Fig.
B. Infection: 24%.
Bacterial superinfection of HC is always secondary to rupture. Usually manifests as a hepatic abscess. US and CT findings are similar to those in other hepatic abscesses. CT shows air forming an air-fluid level inside the hydatid cyst.
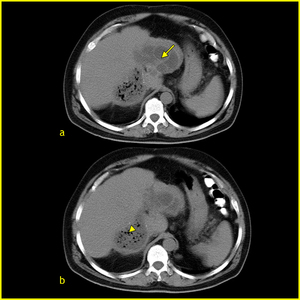
Fig.
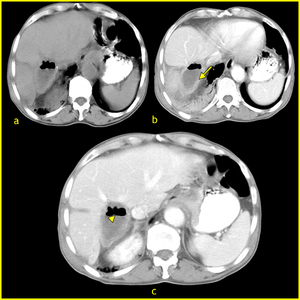
Fig.
2. BILIARY COMMUNICATION 24%
It may occur through small fissures or through a wide perforation that allows access to a main biliary branch. However, dilatation of the biliary tree does not always indicate cyst rupture. The only direct sign of rupture into the biliary tree is the visualization of the cyst wall defect or of a communication between the cyst and a biliary radicle.
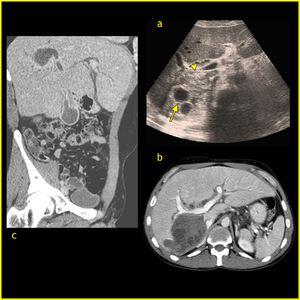
Fig.
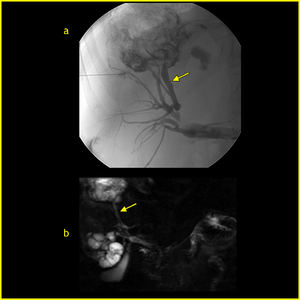
Fig.
3. TRANSDIAFRAGMATIC THORACIC INVOLVEMENT: 9%
Varies from simple adherence to the diaphragm to rupture into the pleural cavity, seeding in the pulmonary parenchyma, and chronic bronchial fistula. Chest radiography may show pleural effusion, elevation of the diaphragm, lung consolidation or laminated atelectasis at the lung bases.
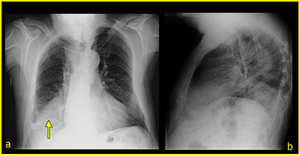
Fig.
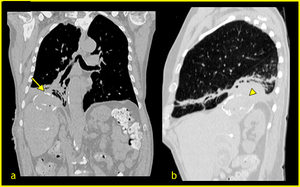
Fig.
4. PERITONEAL SEEDING: 15%
Presence of hydatid material or daugter cyst anywhere in the peritoneal cavity. CT is the modality of choice in affected patients.
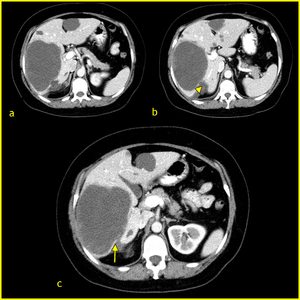
Fig.
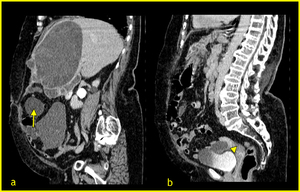
Fig.
5. EXOPHYTIC GROWTH: 12%
Hydatid cysts may use the natural routes provided by the liver capsule, ligaments and peritoneum to progress beyond the boundaries of the liver. The most common routes are the bare area of the liver and the gastrohepatic ligament.
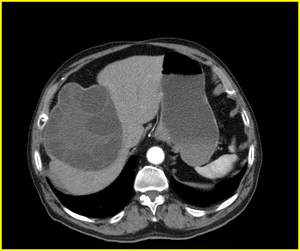
Fig.
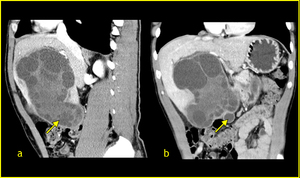
Fig.
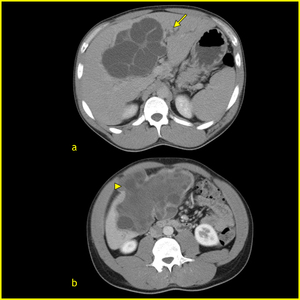
Fig.
Fig.: Please click the image to view the animation.
Video 1. Click here to view the movie
Video 2 Click here to view the movie
6. PORTAL VEIN INVOLVEMENT: 6%
Compression of the portal vein and thrombosis with secondary cavernomatosis are rare and are caused by cysts located in the caudate lobe and hepatic bifurcation.
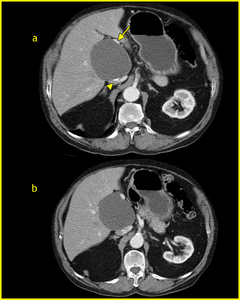
Fig.
7. HEMATOGENOUS DISSEMINATION: 24%
Lungs: are the most frecquent site of hematogenous spread. After cyst rupture, expectoration of cyst fluid, membranes, and scolices may occur. Uncomplicated cysts appears as well-defined masses of different sizes. They can also affect the thoracic wall.
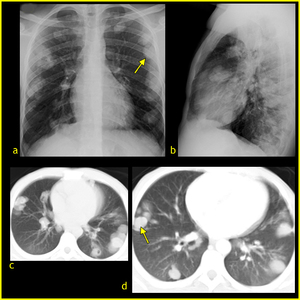
Fig.
Fig.: Please click the image to view the animation.
Spleen: in our serie spleen is the third most common location of hydatid disease involvement after the liver and lungs. Are usually solitary and their imaging characteristics are similar to those of hepatic HC. In the case we show there is also spread to colon.
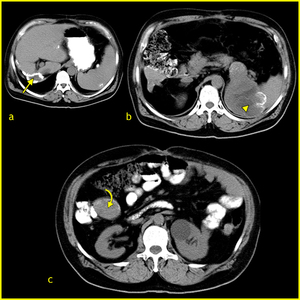
Fig.
Kidneys: cysts are frecuently solitary and located in cortex.
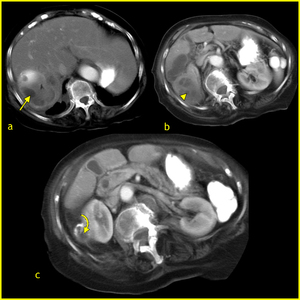
Fig.
Heart: is very rare and may be due to hematogenous spread or rupture of a lung HC. We report two cases.
Fig.: Please click the image to view the animation.
Muscle: muscular involvement is rare. HC can be diagnose with confidence by US or CT when it shows multivesicular lesions but MR may be the most useful imaging tecnique when a complex or solid pattern is present.
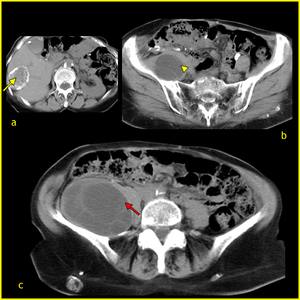
Fig.
