Table-1: centrilobular nodules
| Disease | tree-in-bud nodules | ill-defined nodules |
| HTLV-1* carrier | 88.9 (%) | 11.1 (%) |
| Mycoplasma pneumoniae pneumonia | 84.6 | 7.7 |
| Mycobacterium tuberculosis (Tb) | 73.1 | 25 |
| Mycobacterium avium complex (MAC) | 59.5 | 29.7 |
| Mycobacterium Kansasii | 81.8 | 15.2 |
| Allergic bronchopulmonary aspergillosis (ABPA) | 66.7 | 11.1 |
| Diffuse panbronchiolitis (DPB) | 100 | 0 |
| Follicular bronchiolitis (FB) | 71.4 | 28.6 |
| Diffuse aspiration bronchiolitis (DAB) | 92.3 | 0 |
| Subacute hypersensitivity pneumonitis | 0 | 100 |
| Metastatic calcification | 0 | 100 |
| Alveolar hemorrhage | 5.9 | 55.9 |
| RB-ILD** | 0 | 100 |
HTLV-1*: Human T-cell lymphotropic virus type 1 (HTLV-1) is an etiologic retrovirus of adult T-cell leukemia/lymphoma (ATLL). HTLV-1 carriers were characterized by positive human T-lymphotrophic virus type 1 antibody staining and polyclonal integration of proviral DNA in the peripheral blood or in biopsied tissues.
RB-ILD** : Respiratory bronchiolitis-associated interstitial lung disease
Centrilobular nodules with tree-in-bud appearance were observed in most patients with HTLV-1 carriers, Mycoplasma pneumoniae pneumonia,Tb, MAC, Mycobacterium Kansasii, ABPA, DPB, FB, and diffuse aspiration bronchiolitis.
In patients with mainly tree-in-bud appearance the overwhelming likelihood is that the underlying cause was related to infection, excepting DAB and DPB (Figs. 1-4).
On the other hand, ill-defined centrilobular nodules of GGA were frequently seen in patients with hypersensitivity pneumonitis, metastatic calcification, alveolar hemorrhage, and RB-ILD.
Patients with a centrilobular pattern without tree-in-bud appearance essentially never have underlying infection as an etiology (Figs. 5-7).
Table-2
| Disease | Bronchial wall thickening | Bronchiectasis |
| HTLV-1 carrier | 57.6 (%) | 52.5 (%) |
| Mycoplasma pneumoniae pneumonia | 86.5 | 1.9 |
| Mycobacterium tuberculosis (Tb) | 71.1 | 46.2 |
| Mycobacterium avium complex (MAC) | 73.9 | 59.5 |
| Mycobacterium Kansasii | 57.6 | 54.5 |
| Allergic bronchopulmonary aspergillosis (ABPA) | 77.8 | 77.8 |
| Diffuse panbronchiolitis (DPB) | 83.3 | 83.3 |
| Follicular bronchiolitis (FB) | 71.4 | 71.4 |
| Diffuse aspiration bronchiolitis (DAB) | 92.3 | 30.8 |
| Subacute hypersensitivity pneumonitis | 13.3 | 26.4 |
| Metastatic calcification | 0 | 0 |
| Alveolar hemorrhage | 44.1 | 20.6 |
| RB-ILD | 25 | 0 |
Bronchial wall thickening was frequently seen in patients with mainly centrilobular nodules of tree-in-bud appearance (Figs.1-4).
Bronchiectasis was also frequently seen in those patients (Fig. 3) except those with Mycoplasma pneumoniae pneumonia (Fig. 4).
Bronchiectasis was found in only one patient with Mycoplasma pneumoniae pneumonia.
Histopathologically, this organism targets the ciliated cells of the respiratory tract, while it is characterized by acute cellular bronchiolitis with edematous lesions of the bronchial walls (14,15). Therefore, it is not difficult to understand that the frequency of brochiectasis was lower than those of other subacute or chronic inflammatory diseases with tree-in-bud appearance.
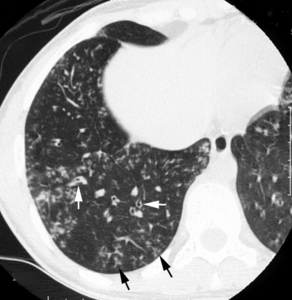
Fig.: Transverse thin-section CT scan (1-mm section thickness) obtained at the level of the right hemidiaphragm shows centrilobular nodules that do not extend to the pleural surfaces, and with tree-in-bud appearance (arrows) with a peripheral distribution. Bronchial wall thickening is also present in the lower lobe (white arrows).
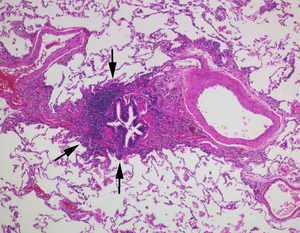
Fig.: Photomicrograph of the surgical biopsy specimen from the right lower lobe shows infiltration by lymphocytes into respiratory bronchioles and alveolar walls (arrows). (Hematoxylin-Eosin, original x 100)
Fig. 1. Images obtained in a 26-year-old woman with HTLV-1.
(a) Transverse thin-section CT scan (1-mm section thickness) obtained at the level of the right hemidiaphragm shows centrilobular nodules that do not extend to the pleural surfaces, and with tree-in-bud appearance (arrows) with a peripheral distribution. Bronchial wall thickening is also present in the lower lobe (white arrows).
(b) Photomicrograph of the surgical biopsy specimen from the right lower lobe shows infiltration by lymphocytes into respiratory bronchioles and alveolar walls (arrows). (Hematoxylin-Eosin, original x 100)
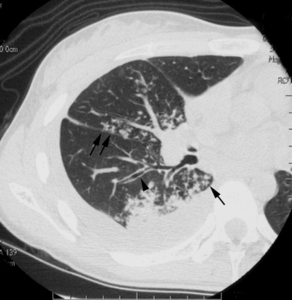
Fig.: Fig. 2. Image obtained in a 21-year-old woman with Mycobacterium tuberculosis.Transverse CT scan (1-mm section thickness) obtained at the level of the division of the middle lobe bronchus shows centrilobular nodules with tree-in-bud appearance (arrows) and bronchial wall thickening (arrowhead). Right pleural effusion is also present.
Fig. 2. Image obtained in a 21-year-old woman with Mycobacterium tuberculosis.
Transverse CT scan (1-mm section thickness) obtained at the level of the division of the middle lobe bronchus shows centrilobular nodules with tree-in-bud appearance (arrows) and bronchial wall thickening (arrowhead). Right pleural effusion is also present.

Fig.: (a) Transverse thin-section CT scan (1-mm section thickness) obtained 2 cm below the division of the right lower lobe bronchus shows centrilobular nodules with tree-in-bud appearance (arrows), bronchial wall thickening, and bronchiectasis (arrowheads). Bronchiolar luminal impaction with mucous is also present (white arrows).
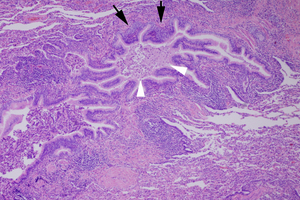
Fig.: (b) Photomicrograph of the surgical biopsy specimen obtained from the right lower lobe shows thickened and dilated terminal bronchioles with mononuclear cell infiltration (arrows) and foamy cells into the alveolar space. Intraluminal secretions are also present (arrowheads). (Hematoxylin-Eosin, original x 100)
Fig. 3. Images obtained in a 16-year-old woman with diffuse panbronchiolitis.
(a) Transverse thin-section CT scan (1-mm section thickness) obtained 2 cm below the division of the right lower lobe bronchus shows centrilobular nodules with tree-in-bud appearance (arrows), bronchial wall thickening, and bronchiectasis (arrowheads). Bronchiolar luminal impaction with mucous is also present (white arrows).
(b) Photomicrograph of the surgical biopsy specimen obtained from the right lower lobe shows thickened and dilated terminal bronchioles with mononuclear cell infiltration (arrows) and foamy cells into the alveolar space. Intraluminal secretions are also present (arrowheads). (Hematoxylin-Eosin, original x 100)
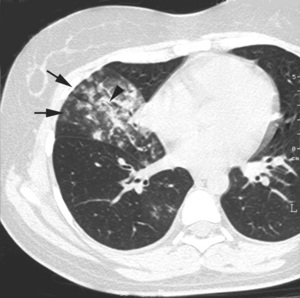
Fig.: Fig. 4. Images obtained in a 25-year-old woman with Mycoplasma pneumoniae pneumonia.Transverse thin-section CT scan (1-mm section thickness) obtained 2 cm below the division of the right lower lobe bronchus shows centrilobular nodules with tree-in-bud appearance (arrows) and bronchial wall thickening (arrowhead). No bronchiectasis is present.
Fig. 4. Images obtained in a 25-year-old woman with Mycoplasma pneumoniae pneumonia.
Transverse thin-section CT scan (1-mm section thickness) obtained 2 cm below the division of the right lower lobe bronchus shows centrilobular nodules with tree-in-bud appearance (arrows) and bronchial wall thickening (arrowhead). No bronchiectasis is present.
Table-3
| Disease | Consolidation | Interlobular septal thickening | Ground-glass attenuation |
| HTLV-1 carrier | 5.1 (%) | 28.3 (%) | 51.5 (%) |
| Mycoplasma pneumoniae pneumonia | 34.6 | 9.6 | 78.8 |
| Mycobacterium tuberculosis (Tb) | 44.2 | 3.8 | 36.5 |
| Mycobacterium avium complex (MAC) | 40.5 | 2.7 | 32.4 |
| Mycobacterium Kansasii | 54.5 | 6.1 | 33.3 |
| Allergic bronchopulmonary aspergillosis (ABPA) | 77.8 | 11.1 | 88.9 |
| Diffuse panbronchiolitis (DPB) | 0 | 0 | 25 |
| Follicular bronchiolitis (FB) | 0 | 57.1 | 71.4 |
| Diffuse aspiration bronchiolitis (DAB) | 15.3 | 30.8 | 76.9 |
| Subacute hypersensitivity pneumonitis | 20 | 20 | 100 |
| Metastatic calcification | 0 | 0 | 25 |
| Alveolar hemorrhage | 54.1 | 26.5 | 91.2 |
| RB-ILD | 0 | 0 | 87.5 |
Consolidation was frequently observed in patients with Tb (44.2%), MAC (40.5%), Mycobacterium Kansasii (54.5%), ABPA (77.8%), and alveolar hemorrhage (54.1%).
Cavitary nodules and cavitary consolidation were observed in patients with Tb (30.8% and 5.8%, respectively), MAC (35.1% and 8.1%, respectively), and Mycobacterium Kansasii (30.3% and 9%, respectively). Cavitary nodules or cavitary consolidation were not observed in patients with other diseases.
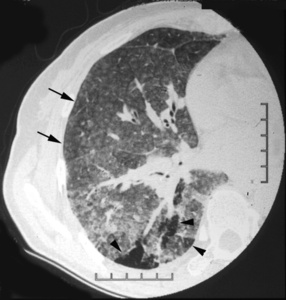
Fig.: (a) Transverse CT obtained 1 cm below the division of the right lower bronchus shows ground-glass attenuation and diffuse ill-defined centrilobular nodules (arrows). Mosaic perfusion is also present (arrowheads).
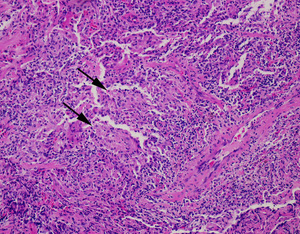
Fig.: (b) Photomicrograph of the surgical biopsy specimen obtained from the right lower lobe shows cellular infiltration along respiratory bronchioles and epithelioid granulomas consisting of spindle cells in peribronchiolar alveolar septa (arrows). (Hematoxylin-Eosin, original x 100)
Fig. 5. Images obtained in a 52-year-old woman with subacute hypersensitivity pneumonitis.
(a) Transverse CT obtained 1 cm below the division of the right lower bronchus shows ground-glass attenuation and diffuse ill-defined centrilobular nodules (arrows). Mosaic perfusion is also present (arrowheads).
(b) Photomicrograph of the surgical biopsy specimen obtained from the right lower lobe shows cellular infiltration along respiratory bronchioles and epithelioid granulomas consisting of spindle cells in peribronchiolar alveolar septa (arrows). (Hematoxylin-Eosin, original x 100)
Pleural Effusions and Lymph Nodes
Pleural effusions were found in patients with Tb (10 of 52) (Fig.2), MAC (6 of 37), Churg-Strauss syndrome (CSS) (2 of 12), and Systemic lupus erythematosus (SLE) (2 of 8). Pleural effusions were mainly found unilaterally, while bilateral effusions were observed in 2 cases with Tb, 1 case with CSS, and 3 cases with Microscopic polyangiitis (MPA).
Mediastinal and/or hilar lymph node enlargement was observed in 7 (13.4%) of Tb, 3 (25%) of DPB, and 2 (28.6%) of FB cases. Enlarged lymph nodes were generally found at the precarinal, paratracheal, tracheobronchial, or subcarinal regions.
Distribution of Disease -Anatomic distribution-
| Disease | Peripheral | Central | Random |
| HTLV-1 carrier | 71.7 (%) | 0 (%) | 28.3 (%) |
| Mycoplasma pneumoniae pneumonia | 59.6 | 5.7 | 34.6 |
| Mycobacterium tuberculosis (Tb) | 71.2 | 1.9 | 26.9 |
| Mycobacterium avium complex (MAC) | 70.3 | 0 | 29.7 |
| Mycobacterium Kansasii | 69.7 | 0 | 30.3 |
| Allergic bronchopulmonary aspergillosis (ABPA) | 0 | 77.8 | 22.2 |
| Diffuse panbronchiolitis (DPB) | 66.7 | 0 | 33.3 |
| Follicular bronchiolitis (FB) | 71.4 | 0 | 28.6 |
| Diffuse aspiration bronchiolitis (DAB) | 100 | 0 | 0 |
| Subacute hypersensitivity pneumonitis | 6.7 | 0 | 93.3 |
| Metastatic calcification | 0 | 0 | 100 |
| Alveolar hemorrhage | 33.8 | 4.4 | 61.8 |
| RB-ILD | 50 | 0 | 50 |
Among patients with diseases whose CT scans showed centrilobular nodules of tree-in-bud appearance, abnormal findings were predominantly seen in peripheral lungs. However, in patients with ABPA, abnormal findings were predominantly seen in central lungs (77.8%).
On the other hand, among patients with diseases whose CT scans mainly showed ill-defined centrilobular nodules, abnormal findings were predominantly randomly distributed (Figs. 5–7).

Fig.: (a) Transverse thin-section CT scan (1-mm section thickness) obtained at the level of the division of the lingular bronchus shows diffuse ill-defined centrilobular nodules (arrows).

Fig.: (b) Tc-99m MDP scintigraphy demonstrates remarkable Tc-99m MDP uptake in bilateral lungs.
Fig. 6. Images obtained in a 46-year-old man with metastatic calcification.
(a) Transverse thin-section CT scan (1-mm section thickness) obtained at the level of the division of the lingular bronchus shows diffuse ill-defined centrilobular nodules (arrows).
(b) Tc-99m MDP scintigraphy demonstrates remarkable Tc-99m MDP uptake in bilateral lungs.
Distribution of Disease -Zonal distribution-
| Disease | Upper | Lower | Random |
| HTLV-1 carrier | 13.1 (%) | 14.1 (%) | 72.7 (%) |
| Mycoplasma pneumoniae pneumonia | 9.6 | 57.7 | 32.7 |
| Mycobacterium tuberculosis (Tb) | 76.9 | 0 | 23.1 |
| Mycobacterium avium complex (MAC) | 51.4 | 13.5 | 35.1 |
| Mycobacterium Kansasii | 60.6 | 3 | 36.4 |
| Allergic bronchopulmonary aspergillosis (ABPA) | 55.6 | 22.2 | 22.2 |
| Diffuse panbronchiolitis (DPB) | 0 | 16.7 | 83.3 |
| Follicular bronchiolitis (FB) | 0 | 57.1 | 42.9 |
| Diffuse aspiration bronchiolitis (DAB) | 0 | 92.3 | 7.7 |
| Subacute hypersensitivity pneumonitis | 60 | 0 | 40 |
| Metastatic calcification | 50 | 0 | 50 |
| Alveolar hemorrhage | 26.5 | 16.2 | 57.3 |
| RB-ILD | 62.5 | 0 | 37.5 |
For predominant zonal distribution, in patients with HTLV-1 and DPB, random distribution was observed in 72 (72.7%) and 10 (83.3%) patients, respectively. In patients with Mycoplasma pneumoniae pneumonia and DAB, lower distribution was observed in 30 (57.7%) and 12 (92.3%) patients, respectively.
In patients with Tb, MAC, Mycobacterium Kansasii, and ABPA, abnormal findings were predominantly seen in the upper zone (76.9%, 51.4%, 60.6%, 55.6%, respectively).
CT and Pathologic Comparison (n=141)
The tree-in-bud appearance represents lymphocytic infiltration distributed along respiratory bronchioles, or bronchiolar luminal impaction with mucous or pus. In addition, the dilated and thickened walls of bronchioles and peribronchiolar inflammation can contribute to the visibility of affected bronchioles with tree-in-bud appearance (Figs. 1b and 3b).
On the other hand, ill-defined centrilobular nodules represent peribronchiolar inflammation or deposition of hemorrhagic materials without the presence of plugging of small airways or dilated bronchioles (Figs. 5b and 7b). These pathologic findings seem to account for the predominant CT findings of ill-defined centrilobular nodules rather than of nodules with tree-in-bud appearance.

Fig.: (a) Transverse thin-section CT (1-mm section thickness) obtained at the level of the division of the right lower bronchus shows ill-defined centrilobular nodules of ground-glass attenuation (arrows). Ground-glass attenuation is also present.
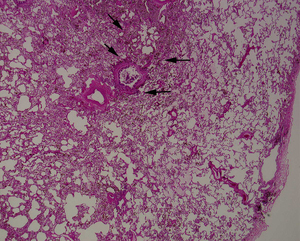
Fig.: (b) Photomicrograph of the surgical biopsy specimen obtained from the right lower lobe shows alveolar hemorrhage and deposition of hemorrhage materials around respiratory bronchioles (arrows). No thickened and dilated bronchial walls are present. (Hematoxylin-Eosin, original x 40)
Fig. 7. Images obtained in a 24-year-old woman with alveolar hemorrhage (SLE).
(a) Transverse thin-section CT (1-mm section thickness) obtained at the level of the division of the right lower bronchus shows ill-defined centrilobular nodules of ground-glass attenuation (arrows). Ground-glass attenuation is also present.
(b) Photomicrograph of the surgical biopsy specimen obtained from the right lower lobe shows alveolar hemorrhage and deposition of hemorrhage materials around respiratory bronchioles (arrows). No thickened and dilated bronchial walls are present. (Hematoxylin-Eosin, original x 40)
