The Parapharyngeal Space (PPS)
This space contains predominantly fat and is surrounded by several other important spaces. It is crescent shaped in its craniocaudal extent. It extends from the skull base to the superior cornu of hyoid thereby allowing spread of infection or tumour between surrounding compartments.
The direction in which fat in PPS is displaced is important in identifying which space a lesion arises from and thereby helps to guide diagnosis.
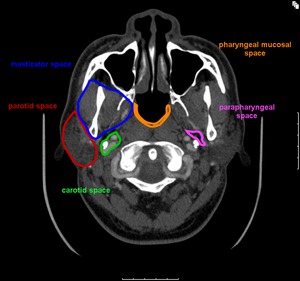
Fig.: Figure 3. Axial CT image illustrating the relationship of the parapharyngeal space and its adjacent compartments
Borders
Medial: pharyngeal mucosal spaces
Lateral: masticator and parotid spaces
Posterior: carotid space
Inferior: communicates with the submandibular space with no intervening fascia
Contents
- Internal maxillary artery
- Ascending pharyngeal artery
It contains NO nodes, mucosa, bone or normal salivary gland tissue - it is therefore unusual for a pathological process to originate from the PPS.
Pathology
Neoplastic
- Pleomorphic adenoma of salivary rest
- Lipoma
- Metastatic disease from surrounding spaces:
-
- Pharyngeal Mucosal Space - SCC - particularly base of tongue, tonsillar fossa and larynx, NHL, minor salivary gland malignancy
- Masticastor Space - sarcoma
- Parotid Space - mucoepidermoid carcinoma, adenoid cystic carcinoma
Non neoplastic
- Atypical second branchial cleft cyst
- Infection - spread from adjacent spaces: eg tonsillitis, parotid calculus disease, odontogenic infection from masticator space
- Asymmetric pterygoid venous plexus
The Pharyngeal Mucosal Space (PMS) Fig. 3
This space is located very superficially along the pharyngeal mucosal walls. It includes the naso and oropharynx medially to the middle layer of deep cervical fascia (buccopharyngeal membrane). The pharyngobasilar fascia is the aponeurosis of superior constrictor muscle attaching it to the skull base. Near the skull base the PMS encloses the lateral and posterior margins of this fascia and more inferiorly, encircles the superior and middle constrictors.
Contents
- lymphoid tissue of Waldeyers’ ring
- pharyngeal constrictor muscles (superior & middle)
- salpingopharyngeus & levator palatini muscles
- cartilaginous part of Eustacian tube
Pathology
Neoplastic
- Benign mixed tumour of minor salivary glands
- SCC (fig. 4 & 5)
- NHL (fig. 6)
- Adenocarcinoma
- Adenoid cystic carcinoma
- Juvenile angiofibroma
Non neoplastic
- Tornwaldt’s cyst
- Tonsillitis, abscess
- Post-inflammatory mucous retention cyst
- Asymmetry of fossa of Rosenmuller
The Masticator Space (MS)
It consists of the muscles of mastication - pterygoids, masseter and temporalis.
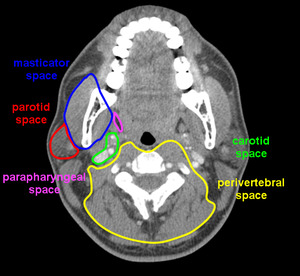
Fig.: Figure 7. Axial CT illustrating the borders of the masseter space and adjacent compartments.
The superficial layer of the deep cervical fascia splits along the inferior border of the mandible to enclose these muscles.
The medial slip courses along the deep edge of pterygoid muscles from the inferior mandible to the skull base.
It inserts medial to the foramen ovale, allowing lesions of MS access to the middle cranial fossa and cavernous sinus via perineural spread along cranial nerve V3.
Superolaterally, the slip of fascia runs over the masseter muscle to the zygomatic arch and to the attachment of temporalis to the outer table of the skull, and so is quite extensive craniocaudally.
Borders
Anterior: Buccal space
Posterior: Parotid space
Posteromedial: Parapharyngeal space
Contents
- Branches of V3, including inferior alveolar nerve
- Ramus and posterior body of mandible
Pathology - Anatomical differential
Muscles of mastication - Mesenchymal lesions
- Benign
- Malignant (commonest in child - rhabdosarcoma, in adult - leiomyosarcoma and malignant fibrous histiocytoma)
- Lymphoma
- Metastases (fig. 8)
- Benign masseter hypertrophy
- Myositis ossificans
Mandibular branch of Trigeminal Nerve (V3)
- Neurogenic tumour eg schwannoma
- Perineural spread of tumour (fig. 9)
Mandible
- Infection - osteomyelitis, odontogenic abscess (fig. 10)
- Metastases
- Myeloma
- Primary bone lesions
Secondary Spread into MS
- Deep spread of SCC from oropharynx
- Caudal extension of intracranial (eg meningioma) or skull base lesions (eg chondrosarcoma)
The Parotid Space (PS) (Fig. 3)
The parotid space is the most lateral space in the suprahyoid neck and is enclosed by the superficial layer of deep cervical fascia.
Borders
Superior: external auditory canal
Inferior: mandible
Medial: parapharyngeal space
Posteromedial: posterior belly of digastric muscle and its fascia (separating it from the carotid space)
The plane of the facial nerve splits the parotid gland into superficial and deep lobes. This is difficult to visualise on routine CT or MR imaging and the retromandibular vein (that lies just medial to facial nerve) is used as a landmark between the deep and superficial lobes.
Contents
- Parotid duct (Stenson's duct)
Pathology
Neoplastic
- Pleomorphic adenoma (fig. 11)
- Warthin's tumour
- Oncocytoma
- Lipoma
- Facial nerve sheath tumour
- Mucoepidermoid carcinoma
- Adenoid cystic carcinoma
- Lymphoma
- SCC
- Metastases to nodes - SCC, melanoma, NHL
Non-neoplastic
- First branchial cleft cyst
- Haemangioma & lymphangioma (in children)
- Abscess or cellulitis
- Lymphoepithlelial cysts
- Reactive adenopathy
The Carotid Space (also known as Carotid Sheath/ Poststyloid Parapharyngeal Space) Fig. 7
All three layers of deep cervical fascia fuse to form the fascia surrounding the carotid space (CS).
It extends from the clivus to the aortic arch. It is tenuous above the level of the hyoid and well formed and tough inferiorly.
Superiorly, it extends to the jugular foramen (as the internal jugular vein enters the posterior cranial fossa) and slightly anterior to the carotid canal for entry of the internal carotid artery into the middle cranial fossa.
Borders
Suprahyoid neck
Anterior: styloid process and PPS
Lateral: posterior belly of digastric muscle and PS
Medial: lateral margin of RPS
Infrahyoid neck
Medial: visceral space
Lateral: sternocleidomastoid
Contents
- Common and internal carotid artery
- Internal jugular vein (IJV)
- Cranial nerves IX, X, XI, XII (only X traverses the entire course of CS from skull base to aortic arch)
Pathology
Neoplastic
- Paragangliomas eg glomus jugulare, glomus vagale, carotid body tumour (fig.12)
- Neural sheath tumour
- Meningioma of jugular foramen
- SCC nodal metastases or direct invasion
- NHL
Non neoplastic - Carotid artery ectasia or aneurysm
- Thrombosed IJV
- Carotid space cellulitis
The Retropharyngeal Space (RPS)
It is a potential space that lies between pharyngeal constrictor muscles anteriorly and prevertebral muscles posteriorly and is usually seen as a line of fat. It is between the middle and deep layers of the deep cervical fascia.
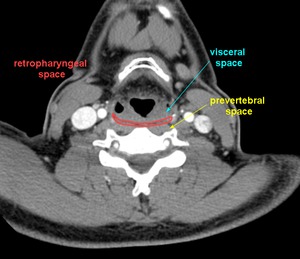
Fig.: Figure 13. Axial CT illustrating the retropharyngeal space.
The lateral walls are made up of a slip of deep cervical fascia (alar fascia). Another slip of deep fascia divides the RPS into an anterior (true RPS) and posterior compartment.
The posterior compartment is known as the Danger space (DS) which extends from the skull base to the diaphragm, and acts as a pathway into the posterior mediastinum.
Radiologically, lesions of the RPS and DS are otherwise indistinguishable.
Borders
Anterior: pharyngeal mucosal space
Posterior: perivertebral space
Lateral: carotid space
Contents
- Lateral lymph nodes/ nodes of Rouviere (usually high in oro and nasopharynx)
- Medial lymph nodes (not normally visible on CT/MRI; if present assumed pathological)
- No nodes below the level of the hyoid in RPS
Pathology
Is within the RPS regardless of size if it is anterior to the prevertebral muscles.
Neoplastic
- Lipoma
- Nodal metastases (commonly from naso, oro & hypopharynx & nasal cavity)
- Nodal NHL
- Direct invasion from adjacent SCC
Non neoplastic
- Haemangioma, lymphangioma
- Reactive adenopathy
- Cellulitis / abscess (fig 14 & 15)
The Perivertebral Space (PVS)
Enclosed by a deep layer of deep cervical fascia that runs from the transverse process of each cervical vertebra anteriorly to the opposite transverse process. This lateral attachment divides it into anterior (prevertebral) and posterior (paraspinal) compartments.
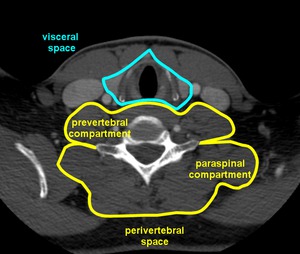
Fig.: Figure 16. Axial CT illustrating the perivertebral and visceral spaces.
Posteriorly, it encases the paraspinal muscles and attaches to the nuchal ligament.
It is a tough fascia with only the roots of the brachial plexus (C5 - T1) piercing it.
Features suggesting involvement of PVS are:
- vertebral body involvement
- displacement the retropharyngeal space anteriorly
- displacement of the contents of the carotid space laterally
- displacement of the posterior wall of the pharyngeal mucosal space
- anterior elevation of the prevertebral muscles
As it is a tough fascia, primary lesions are usually confined within this space and can lead to epidural spread.
Pathology
Neoplastic
- Neural sheath tumour
- Chordoma
- Vertebral body metastases (fig. 17), epidural metastases
- Lymphoma
- Direct extension of carcinoma from nasopharynx
- Primary bone tumour
Non-neoplastic
- Vertebral body osteomyelitis
- Vertebral disc herniation (anterior)
- Cervical rib
- Vertebral osteophyte
- Levator scapulae hypertrophy
The Visceral Space (VS) Fig. 18
The middle layer of the deep cervical fascia encloses this space that runs from the hyoid to the mediastinum.
Contents
- Thyroid & parathyroid glands
- Hypopharynx, larynx, trachea
- Recurrent laryngeal nerve
A malignant visceral space lesion leads to loss of the soft tissue planes between the structures within it. (fig. 19)
The Posterior Cervical Space (PCS)
This extends from the skull base to the clavicles and is between the superficial and deep layers of the deep cervical fascia. The carotid sheath lies anteriorly. Its main volume lies within the infrahyoid neck.
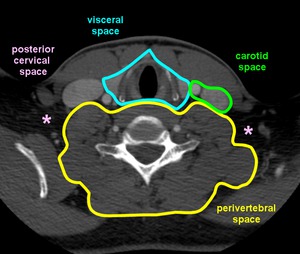
Fig.: Figure 20. Axial CT illustrates the posterior cervical space (pink*) and its neighbouring spaces.
Contents
- Spinal accessory lymph node chain
- Preaxillary brachial plexus
A lesion arising within this space must have its centre within the fat of the PCS. A thin slip of fat often separates the mass from the carotid space anteriorly. Superiorly, the carotid space and PCS are in close relation to each other and unless fat is present between the mass and the carotid space, the lesion should be thought to be arising from the carotid space and not the posterior cervical space. (fig. 20)
LYMPH NODES
Lymph nodes are an important structure within the head and neck, and knowledge of the normal appearance and location is vital. Presence of abnormal nodes can guide and aid the radiologist and clinicians to the primary site of pathology.
Lymph nodes are considered abnormal when:
- ≥ 1.5cm in the jugulo-digastric region, ≥ 1cm in short axis diameter elsewhere
- necrotic, regardless of size
- they have ill defined borders as there may be extracapsular extension with infiltration of the surrounding fat planes or encasement of vessels such as the carotid.
Nodal Groups and Metastatic Disease:
Supraclavicular
- metastasis from any source, but lung, breast and oesophagus are most common
Inferior jugular chain
- supraglottic larynx, oesophagus, or thyroid
Midjugular
- tongue, pharynx, or supraglottic laryngeal cancers
Jugular digastric region
- pharynx, tonsil, tonsilar fossa, tongue, parotid gland, or supraglottic larynx
Submandibular region
- adjacent skin, submandibular gland or base of the tongue carcinoma
